
Abstract
Background
Small scale shared housing arrangements (SHAs) is a deinstitutionalized model of care designed to resemble a typical home of <10 people and are increasingly available for persons with neurocognitive disorders of the Alzheimer's and related types (NCD). However, there is little aggregate evidence of their effect on persons with NCD thus, a literature review was performed.
Methods
Database searches were conducted across CINAHL Complete, OTseeker, PubMed, Ovid, Academic One File, ProQuest Nursing and Allied Health, the World Wide Web and Google Scholar using the several key words that included neurocognitive disorders, Alzheimer's, dementia, quality of life, well-being, occupational performance, activities of daily living, small scale shared housing, sheltered housing and group homes. Bibliographic references from final articles were also examined. Selection criteria involved three steps: screening perspective articles by title and abstract, assessing full text for eligibility and finally, reviewing full-texts.
Results
16 studies were selected for final review where most found the association of SHAs with various occupational performance indicators unique to the NCD population better than or equal to controls (traditional models of long term care). A small minority of studies had mixed or inconclusive results. No study found SHAs necessarily worse than controls.
Conclusion
The SHA model has many benefits for person's with NCD and may be especially advantageous for those in the early stages of the disease process. The occupational therapy profession should continue to raise awareness of SHAs and consider ecological theory as a valid basis for their expansion.
Introduction
Background
Numerous issues are confronting the provision of long-term rehabilitative care (LTC) and its effect on quality of life (QpL) for those with neurocognitive disorders of the Alzheimer's and related types (NCDs); given that physical health and function are its intended outcomes, LTC (a parasol term for nursing homes, assisted living, skilled nursing, and similar facilities) has come to be associated with isolation from the community, loss of autonomy, poor occupational performance, and reduced QpL (
SHAs are not necessarily new and made their debut in the early 1980s in Scandinavian countries, Japan, and Germany. Representing a novel concept in NCD care at that time, they now account for >25% of all nursing home care in the Netherlands and as of 2008 represented 18% of the total 6,000 special care nursing homes in Japan (
Occupational therapy is at a unique crossroad with those who suffer from NCD as the number of cases in the United States is expected to rise dramatically by the year 2050, with estimates suggesting 14 million people to be affected by the disease, of which 7.0 million will be >85 years (
Literature review
The looming NCD crisis proposed by the anticipated shift from 5 million to 14 million cases by 2050 is creating a unique opportunity for today's occupational therapy professionals to not only affect but also guide the debate relative to the expansion of the SHA model of care, as construction of new LTC beds is projected to expand at an annual compound growth rate of 8% over the next decade. Thus, significantly additions are projected to be made to the current 15,700 nursing homes and 22,200 assisted living and similar residential care communities currently in the United States (
Characteristics of Selected Articles for the Literature Review.
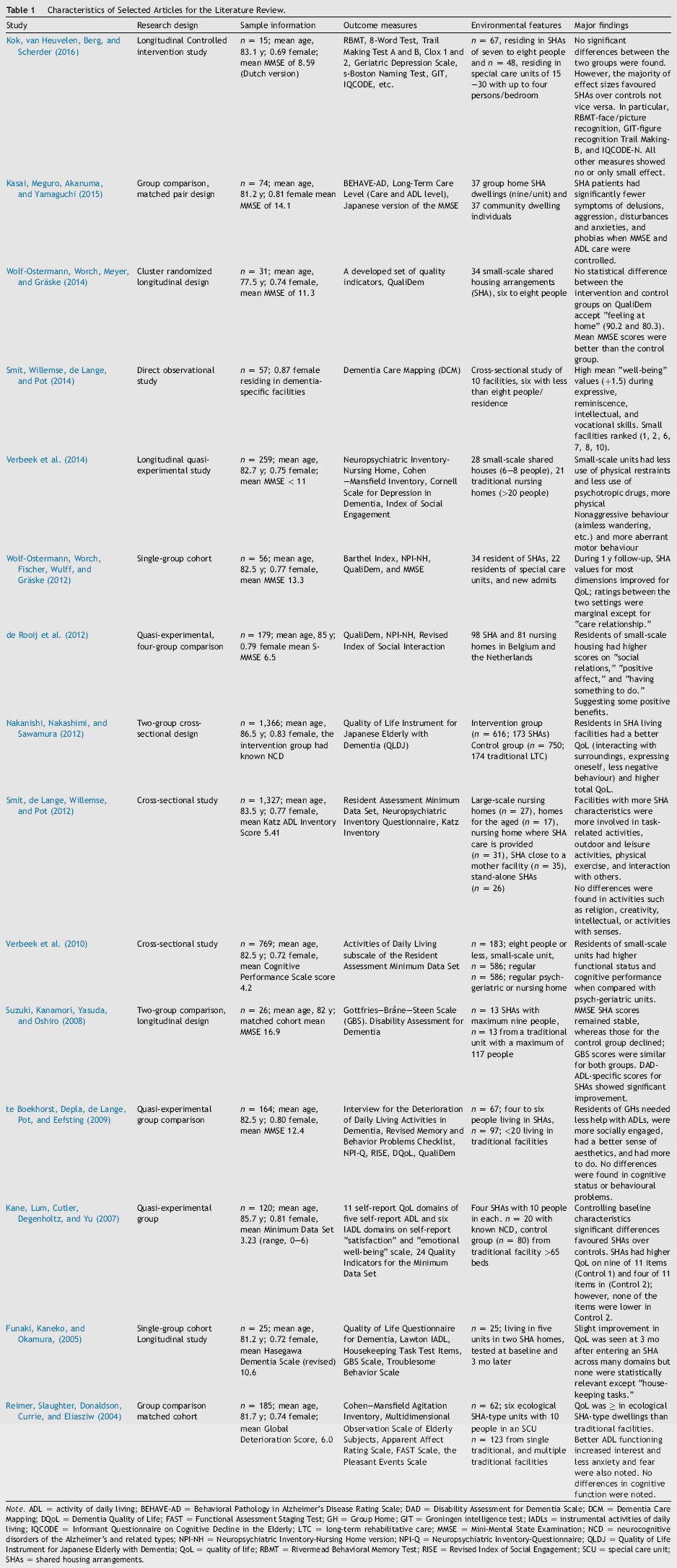
Note. ADL = activity of daily living; BEHAVE-AD = Behavioral Pathology in Alzheimer's Disease Rating Scale; DAD = Disability Assessment for Dementia Scale; DCM = Dementia Care Mapping; DQoL = Dementia Quality of Life; FAST = Functional Assessment Staging Test; GH = Group Home; GIT = Groningen intelligence test; lADLs = instrumental activities of daily living; IQCODE = Informant Questionnaire on Cognitive Decline in the Elderly; LTC = long-term rehabilitative care; MMSE = Mini-Mental State Examination; NCD = neurocognitive disorders of the Alzheimer's and related types; NPI-NH = Neuropsychiatric Inventory-Nursing Home version; NPI-Q = Neuropsychiatric Inventory-Questionnaire; QLDJ = Quality of Life Instrument for Japanese Elderly with Dementia; QoL = quality of life; RBMT = Rivermead Behavioral Memory Test; RISE = Revised Index of Social Engagement; SCU = special care unit; SHAs = shared housing arrangements.
Methods
A database search was conducted across CINAHL Complete, OTseeker, PubMed, Ovid, Academic OneFile, ProQuest Nursing and Allied Health, the World Wide Web, as well as Google Scholar using the following keywords: neurocognitive disorder(s), Alzheimer's, dementia, fronto-temporal, Lewy body(ies), vascular, quality of life, well-being, occupational performance, activities of daily living, ADLs, small scale shared housing, SHAs, special care facility, sheltered housing, and group home. Bibliographic references from final articles were also examined to provide further insight into the topic. The comprehensive search returned >4,000 articles, of which 240 citations met initial inclusion criteria. Stepwise screening of the 240 articles yielded 85 papers that were inspected in detail and graded on their ability to meet designated conditions outlined by
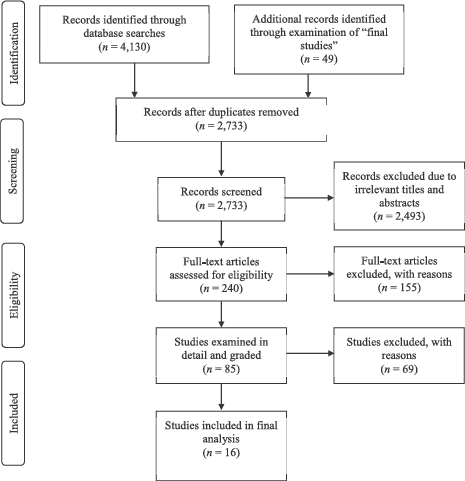
Flow diagram of studies included in final review.
Analysis of final articles
Arguably, most people would prefer to age in place but often there is a need for medical, physical, and occupational therapy services beyond the scope of the home that can only be delivered in a rehabilitative setting when an individual is no longer able to meet the occupational demands of their living environment. Advocating what setting is most appropriate for client and client populations is an important aspect of the profession because a transition to a new environment can affect established roles, as well as routines and meaningful occupations (
A hallmark of the disablement process posed by NCD often includes an array of heterogeneous neuropsychiatric symptoms such as delusions, hallucinations, agitation, aggression, depression, apathy, euphoria, anxiety, disinhibition, irritability, and aberrant motor behaviour, which may necessitate the need for the prescription of psychotropic drugs, and as much as 69% of all nursing home residents are prescribed at least some type of medication (
The last major theme of the LR revolves around cognitive impairment where its diagnosis suggests evidence of significant decline from a previous level of performance in one or more domains such as complex attention, executive function, learning and memory, language, perceptual-motor, or social cognition such that those deficits interfere with ADL engagement that has preferably been documented through standardized neuropsychological testing (
Results
Findings of the LR propose that SHAs have many advantages for the NCD population when compared with traditional LTC facilities as most studies found incremental improvement across many performance indicators unique to the NCD population. Although none showed definitively that they were better than controls, there was a tendency in the direction of better performance (objectively assessed and subjectively observed) in most studies (
Ecological framework
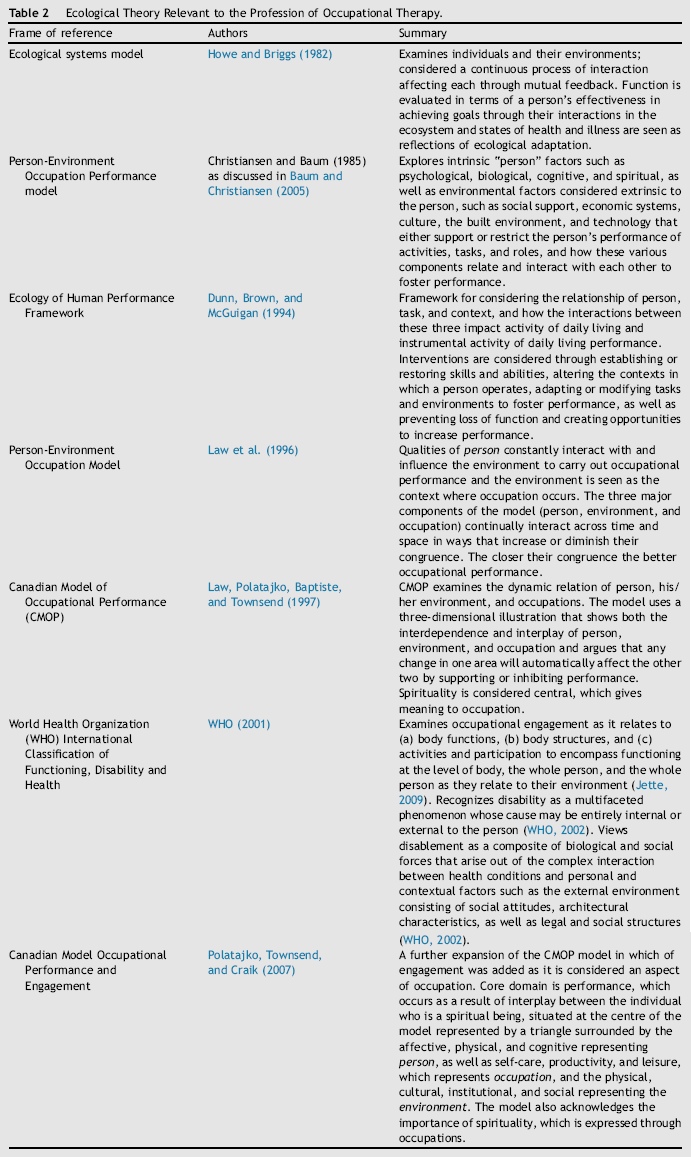
The occupational therapy profession and other stakeholders should approach the proposed development of SHAs from the understanding of an ecological model because it recognizes that disability created the moment a person with a pathological condition or injury interacts with an environment that does not support occupational performance because occupation, for those with NCD, is known to affect a person's well-being including positive affect, less depressive symptoms, elevated interest and alertness, less boredom, higher nutrition intake, and decreased use of psychotropic medications (
Ecological Theory Relevant to the Profession of Occupational Therapy.
Conclusion
For individuals associated with the occupational therapy profession who are constrained by working environments that do not support client health and well-being, a desire for occupational justice exists. A concept that involves the recognition that an inequality in service delivery may be occurring and instills an aspiration for fairness and equal opportunity without discrimination based on disability and includes a social commitment to universal design and accessibility is necessary, enabling people with NCD to flourish to their greatest potential throughout their remaining lifespan (
Limitations
Although this paper raises awareness of both the issues and opportunities that face the profession of occupational therapy as it relates to LTC for those with NCD, it is limited in its presentation of peer-reviewed research, suggesting that alternative means of gathering and presenting evidence might better advance the breadth and detail of the evidence to the clinician, administrator, or policy maker. For example, a systematic review (SR), which through its construct, delivers a more comprehensive analysis of the full range of literature of a subject. This is achieved by utilizing a rigorous and structured approach to searching, examining, appraising, and summarizing information not seen in the LR. The resulting SR method is thus more inclusive and less biased. Examination of the minutiae details of each database can be a meticulous and time-consuming process; for example, Medline bibliographic alone contains >22 million references, of which approximately 750,000 references were added in 2014 (