
Abstract
Objective/Background
This longitudinal study explored factors influencing the rehospitalisation of patients with schizophrenia in Japan.
Methods
Participants comprised patients with schizophrenia who were discharged from a psychiatric hospital in Japan. The investigations were conducted at the time of discharge and one year later. Demographics and clinical characteristics included the following: the type of occupational therapy (OT) interventions (group and individualized or group only); the assessment scales’ scores on hospitalisation; the community living conditions after discharge; and the contents of outpatient treatment (outpatient OT, day-care treatment, home-visit nursing, and adherence to outpatient treatment and medication). All variables were examined in a binomial logistic regression analysis to identify the factors for rehospitalisation.
Results
The rehospitalisation rate was 31.8%, as 14 of 44 participants were rehospitalised within one year after discharge. The type of OT interventions (OR = 7.05, 95% CI = 1.36 −36.69, p = .020) and the adherence to outpatient treatment and medication (OR = 9.48, 95% CI = 1.82–49.33, p = .008) were significant contributing factors to rehospitalisation.
Conclusion
This study provided preliminary support for the finding that individualized occupational therapy and proper adherence to outpatient treatment and medication are associated with reducing the rehospitalisation of patients with schizophrenia in Japan.
Introduction
Of the psychiatric inpatients in Japan in 2014, 62% were patients with schizophrenia, and the majority of these were repeated cases of hospitalisation (
The rehospitalisation rate is an important indicator of psychiatric care outcome; therefore, it is necessary to investigate the factors associated with rehospitalisation to improve the quality of psychiatric care. Previous studies in countries other than Japan have reported that various factors such as sex (
In Japan,
We previously developed the individualized OT programme (IOT) and examined its effects on neurocognition, symptoms, and social functioning of patients with schizophrenia at a hospital setting (
The IOT consisted of a combination of effective psychosocial treatment programmes: motivational interviewing, self-monitoring, individualized visits, handicraft activities, individualized psychoeducation, and discharge planning (Table 1). Motivational interviewing (
Summary of the Individualized Occupational Therapy Programme.
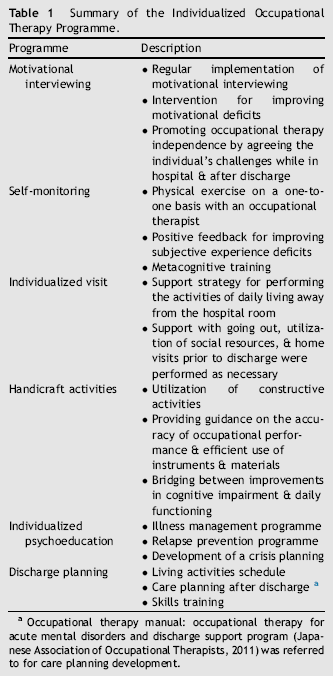
Occupational therapy manual: occupational therapy for acute mental disorders and discharge support program (Japanese Association of Occupational Therapists, 2011) was referred to for care planning development.
Constructive handicraft activities with clear procedures and good feasibility such as Japanese paper collages, plastic models, Japanese paper crafts, and jigsaw puzzles were used in the IOT. In order to promote cognitive functioning, the patients were asked to attend to, concentrate on, precisely perform, and efficiently use the craft tools. Occupational therapists implemented interventions bridging improvements in cognitive impairment and daily functioning (
The GOT was activity-oriented group treatment implemented on a weekly basis. GOT included the following programmes: a physical fitness programme (stretching exercises and relaxation techniques); a handicraft activities programme, where participants choose and make desired activities programmes; a cooking programme; a music programme (music appreciation and singing); a recreation programme; and a group psychoeducation programme. The participants voluntarily selected any desired programme among these. These programmes were held either in hospital wards or in OT departments; from 10 to 15 patients simultaneously participated in each programme.
The previous findings provided preliminary support for the effectiveness of the IOT in improving neurocognition and symptoms in patients with schizophrenia. However, the impact of OT interventions on the rehospitalisation of patients with schizophrenia have not yet been evaluated.
Therefore, we conducted this longitudinal study to explore factors influencing the rehospitalisation of patients with schizophrenia in Japan, including the OT interventions, and examined whether IOT was associated with reducing rehospitalisation rates among patients with schizophrenia in Japan.
Methods
This longitudinal study evaluated factors influencing the rehospitalisation of patients with schizophrenia who were discharged from a psychiatric hospital in Japan. This study was conducted between January 2010 and November 2013 at the Mental Support Soyokaze Hospital, Nagano, Japan. This study was approved by the Ethics Board of the Mental Support Soyokaze Hospital. Study participants provided their written informed consent for all study procedures.
Participants
The inclusion criteria for this study were: age 20—65 years, recently hospitalized patients in a psychiatric hospital and discharged within 1 year, and having a diagnosis of schizophrenia or schizoaffective disorder according to the Structured Clinical Interview for DSM-IV-TR criteria (
Measurements
Demographics at discharge included age, sex, age of onset, number of hospital stays, total length of hospital stay, marital status, experience of work, OT experience, length of time to start OT after hospitalisation, length of last hospital stay, length of OT interventions, type of OT interventions (GOT and IOT or GOT only), and antipsychotic medication (chlorpromazine equivalent dose). This information was drawn from medical records.
Assessment scores were also drawn from medical records. These included the Brief Assessment of Cognition in Schizophrenia—Japanese version (BACS-J;
We investigated community living conditions after discharge (whether receiving support at home or in a facility), source of income (salary, utilization of disability pension or welfare, and pecuniary assistance from family), and outpatient treatment content (outpatient OT, day-care treatment, and home-visit nursing, and adherence to outpatient treatment and medication) through a 1-year follow-up after discharge. The psychiatrists in-charge obtained information from participants, support persons, and visiting staff concerning adherence to outpatient treatment and medication, and made determinations based on regular hospital visits without interruptions or self-adjustment of medications within 1 year following discharge.
OT interventions
The IOT aimed at facilitating proactive participation in treatment and improving functional outcomes. It consisted of a combination of effective psychosocial treatment programmes: motivational interviewing, self-monitoring, individualized visits, handicraft activities, individualized psychoeducation, and discharge planning. In addition, some of its components were very relevant to OT practice. The IOT was provided on a one-on-one basis with the occupational therapist in-charge of the case during hospitalisation and was tailored to each participant. Therapeutic structure factors such as time, frequency, and place were set for each individual.
The GOT was made up of activity-oriented group programmes. The participants voluntarily select any desired programme among those that were available. Time and frequency of the OT programmes for both the GOT + IOT and GOT alone groups were adjusted according to recovery condition; however, these were generally for 1—2 hours at a time and from three to five times per week. Notably, more than half of the OT time was devoted to IOT in the GOT + IOT group. Our previous study (
Procedures
This longitudinal study recruited participants based on referrals from their occupational therapists. These therapists started recording OT interventions and measurements in 1-year follow-up after discharge and outpatient phases. Eligible participants were assigned to groups based on whether they were or were not rehospitalised at the 1-year follow-up. The time points of the investigation were at discharge and at 1 year following discharge. Baseline data at discharge were drawn from medical records, which included information of demographics, BACS-J, PANSS, and GAF scores, and antipsychotic medication taken during hospitalisation. Follow-up data at 1 year after discharge were obtained for each participant regarding community living conditions after discharge and outpatient treatment content at outpatient hospital visits throughout the follow-up period. The occupational therapists and psychiatrists in-charge of the case collected this information.
Statistical analyses
First, we made between-group comparisons of the demographics; the scores of the BACS-J, PANSS, and GAF measures of hospitalisation; the community living conditions after discharge; and the contents of outpatient treatment using t tests for continuous variables and χ2 analyses for categorical variables. Variables that satisfied the significance condition p < .05 were selected for further analysis using logistic regression analysis. Second, we calculated Pearson's correlation coefficient between each variable that had significant differences in the previous univariate analyses in order to exclude the influence of multicollinearity, for variables with r > .4. Third, we conducted a binomial logistic regression analysis to determine the factors influencing rehospitalisation and to calculate the odds ratio (OR) and 95% confidence interval (95% CI) after controlling simultaneously for potential confounders, with rehospitalisation as the dependent variable and the variables that were selected in previous analyses as the independent variable. Statistical analyses were performed with Ekuseru—Toukei 2010 (Social Survey Research Information Co., Ltd., Tokyo, Japan). The level of significance was set at p < .05.
Results
Demographics at discharge are shown in Table 2. The number of recently hospitalized patients with schizophrenia was 72. Of these, 51 met the inclusion criteria and participated in our previous study, and seven were excluded from the analyses. Five patients had > 1 year of hospitalisation, and two patients emigrated to other regions after discharge; therefore, 44 patients were included in the final analyses.
Comparison of the Demographics and Clinical Characteristics of Patients who were and were not Rehospitalised.
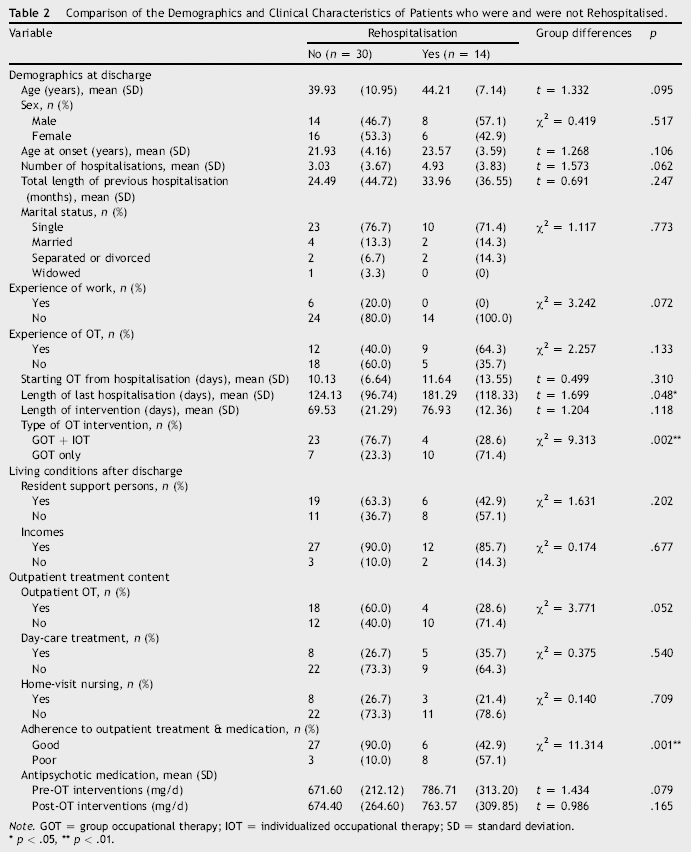
Note. GOT = group occupational therapy; IOT = individualized occupational therapy; SD = standard deviation.
p < .05
p < .01.
The rehospitalisation rate was 31.8%, as 14 participants were rehospitalised within 1 year after discharge. Participants who were not rehospitalised demonstrated a significantly shorter length of last hospital stay (t = 1.70, p = .048), received more IOT during their hospital stay (χ2 = 9.31, p = .002), and had better adherence to outpatient treatment and medication after discharge (χ2 = 11.31, p = .001) compared to the participants who were rehospitalised.
BACS-J, PANSS, and GAF scores concerning hospitalisation are shown in Table 3. There were no significant differences in the assessment scales' scores between participants who were not rehospitalised and those who were before the OT intervention. Participants who were not rehospitalised demonstrated significant improvements in verbal fluency on the BACS-J (t = 1.90, p = .032) compared to those who were rehospitalised at discharge.
Comparison of BACS-J, PANSS, and GAF Scores Before Hospitalized OT and at Discharge among Patients who were and were not Rehospitalised.
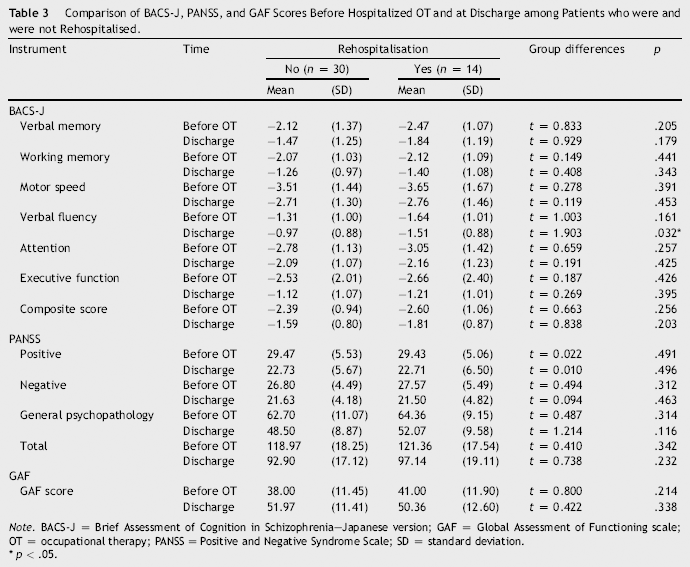
Note. BACS-J = Brief Assessment of Cognition in Schizophrenia—Japanese version; GAF = Global Assessment of Functioning scale; OT = occupational therapy; PANSS = Positive and Negative Syndrome Scale; SD = standard deviation.
p < .05.
The correlation between variables including length of last hospital stay, type of OT interventions, adherence to outpatient treatment and medication, and verbal fluency at discharge showed significant differences in univariate analyses (Table 4). There was a significant positive but mild correlation of adherence to outpatient treatment and medication and verbal fluency at discharge (r = .324). Therefore, all these variables were used as independent variables for a binomial logistic regression analysis.
Pearson's Correlations of Variables with Significant Differences among the Demographic and Clinical Variables (n = 44).
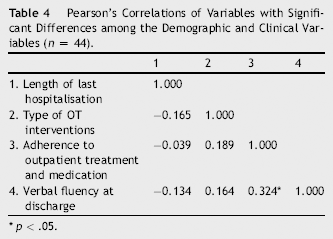
p < .05.
The results of a binomial logistic regression analysis with rehospitalisation as the dependent variable and the length of last hospital stay, type of OT interventions, adherence to outpatient treatment and medication, and verbal fluency at discharge as the independent variables are shown in Table 5. The type of OT interventions (OR = 7.05, 95% CI = 1.36, 36.69, p = .020) and the adherence to outpatient treatment and medication (OR = 9.48, 95% CI = 1.82, 49.33, p = .008) significantly contributed to rehospitalisation over 1 year after discharge.
Odds Ratios (OR) and 95% Confidence Intervals (CI) for Rehospitalisation Associated with Demographics and Clinical Variables Following Discharge (n = 44).
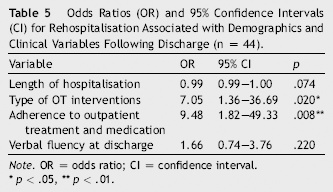
Note. OR = odds ratio; CI = confidence interval.
p < .05
p < .01.
Discussion
The main finding of this study is that the type of OT intervention and the adherence to outpatient treatment and medication were factors influencing the rehospitalisation of patients with schizophrenia within 1 year after discharge from a psychiatric hospital. This study provides preliminary support for the idea that IOT is useful for the prevention of rehospitalisation, in addition to supporting positive adherence to outpatient treatment and medication. To the best of our knowledge, this is the first study to show that IOT is useful in preventing the rehospitalisation of patients with schizophrenia in Japan.
The current rehospitalisation rate (31.8%) was comparable to that of previously published studies in Japan using similar methodologies (33.4%,
One intriguing finding is that the type of OT interventions (GOT + IOT or GOT only) was found to be a significant contributing factor to rehospitalisation. Therefore, IOT may be effective at preventing the rehospitalisation of patients with schizophrenia. The IOT consisted of a combination of motivational interviewing, self-monitoring, individualized visits, handicraft activities, individualized psychoeducation, and discharge planning. It was not possible to identify clearly how or what components of the IOT prevented rehospitalisation in this study design. However, the overall findings may provide useful avenues for future studies and for clinical implications.
We previously reported that IOT was effective at improving the cognitive impairment experienced by patients with schizophrenia (
Previous studies have reported that psychoeducation and discharge planning, which constitute part of the IOT, are useful for improving insight and treatment adherence and may help prevent rehospitalisation in patients with schizophrenia (
A number of limitations should be noted. First, participants included only patients with schizophrenia who were discharged within 1 year after hospitalisation; therefore, long-term inpatients with > 1 year of hospitalisation were not included. Consequently, the factors influencing the rehospitalisation of long-term inpatients should be investigated further. Second, there is a need for more long-term follow-up in future studies, because the follow-up length was only 1 year after discharge in this study. Third, there is a need for a randomized controlled trial design for the GOT+IOT versus the GOT alone group to reduce selection biases and more vigorously examine the relationship between IOT and rehospitalisation, because our previous study design was a non-randomized controlled trial in which group allocation was based on voluntary selection according to the participants' preferences. Fourth, the lower rehospitalisation rate among those who received GOT + IOT might be due to the cumulative effect of both GOT and IOT, not only IOT alone, because this study design did not implement measurements at 1 year after discharge. Therefore, it is necessary to investigate these issues with a study design that partials out the effect of GOT. Fifth, this study's results are limited because it was a single-site study, and the sample size was small. Therefore, it is necessary to investigate other factors for rehospitalisation, including community mental health services, with a larger number of patients with schizophrenia in a multicentre study.
Conclusion
This study investigated factors influencing the rehospitalisation of patients with schizophrenia after discharge from a psychiatric hospital in Japan. Results revealed that the type of OT interventions and the adherence to outpatient treatment and medication were significant contributing factors to rehospitalisation. This study also provided preliminary support for the effects of IOT on reducing rehospitalisation of patients with schizophrenia in Japan.
Footnotes
Acknowledgements
The authors thank all of the participants involved in this study. We also thank the Mental Support Soyokaze Hospital for their support with this study.