
Abstract
This paper analyzes patterns of tips, gifts and bribes paid by patients for health care services. Informal payments are more prevalent in developing and transition countries because the economic and socio-cultural environment is more conducive to “gifts”-exchange as a means to maintain the underfunded health care system. Moreover, most Eastern European countries have experienced wider socio-political reforms, which have also affected health care service provision and have led to a greater reliance on informal patient payments in the access and quality assurance of health care services. This study provides evidence on public attitudes and recent experiences with informal patient payments in post-Soviet and post-communist countries, namely in Lithuania, Ukraine and Poland. The empirical results suggest a lower share of informal patient payments as well as a prevalence of more negative attitudes towards informal patient payments in Poland compared to Lithuania and Ukraine. Informal payments are more common and more expensive for in-patient health care services in contrast to out-patient ones in all countries. Still, in post-Soviet Lithuania and Ukraine informal patient payments co-exist with other types of patient payments such as quasi-formal patient payments. When clear regulation of the basic package and formal patient charges is lacking, patients experience a mixture of payment obligations. About three quarters of the respondents support the statement that informal patient payments should be eradicated. It is proposed therefore that governments of the countries should meet public expectations and implement a strategy to deal with informal patient payments. In all three countries, informal patient payments (both “bribes and fees”) are a symptom of system failure and provide a means for patients to obtain the health care they desire, which the government is not able to guarantee. Suitable regulations coupled with (dis)incentives may decrease the level of informal payments for health care provision.
Introduction
In post-communist countries, including post-Soviet European countries, informal payments given by grateful patients to health care providers have been observed to exist since the 1970s (Gaal, 2004; Mossialos, Dixon, Figueras, & Kutzin, 2002). However, the phenomenon of informal payments emerged much earlier and existed in Western European countries as well. In the past, it was common that patients brought in-kind donations for their family doctors on a regular basis in order to show thankfulness for their work (Adam, 1985, 1986 in Gaal & McKee, 2005; Levene & Sireling, 1980). As Winslow (1946, p. 316) noticed over sixty years ago, “the tribute from one g.p. (the grateful patient) to another g.p. (the general practitioner) is a supplement to – not a substitute for – an assured income”. In Western European countries, the phenomenon diminished or even disappeared as a result of a drive towards more transparency, accountability and control, and greater emphasis on professional norms and conduct (Bovi, 2003; Stone, 1997; Williams, 2005). Health care reforms, i.e. most notably the introduction of universal and generous health insurance systems, which ensured physicians of a stable and adequate income, also contributed to that (Bass & Wolfson, 1980; Greenberg, 1990; Orentlicher, 1994). Meanwhile, informality in the patient–physician relation flourished in the Soviet context.
Until the 1990s, market regulatory mechanisms such as negotiable prices and competition were not applied in communist and Soviet countries due to the existing socio-political arrangements. Indeed, the low public health care funding in post-Soviet republics (in the absence of private spending) led to insufficient health care resources and inequalities in access to public services and goods. Hence, a variety of informal strategies dominated in health care and other “non-productive” sectors (Ensor, 2004). Indeed, “blat” (the attainment of public goods through personnel connections often anchored in long-term social relationships) became a ruling approach in social life and relations (Ledeneva, 1998; Patico, 2002; Rivkin-Fish, 1997; Salmi, 2003). Because of shortages in goods (rather than money) during the communist or Soviet period, informal payments in the form of gifts like perfumes and alcohol, were especially appreciated in contrast to cash payments. The health care sector was no exception to the “ideologies of gift exchange” (Patico, 2002, p. 346). Similarly to other sectors, e.g. education, police, courts of justice and custom offices (Ledeneva, 2006; Miller, Grødeland, & Koshechkina, 1998), gifts and barter supported by reliable connections dominated in health care provision. Patients relied on these strategies mainly to motivate the underpaid health care staff and to receive extra attention of the staff. However, certain restraints were perceptible due to the strong punishment system during the Soviet period (Heinzen, 2007; Wanner, 2006). Also, when the provider is not interested in monetary transactions, gifts and favors exchanged and regulated by complex rules of reciprocity (Granovetter, 2007) may become an important but still rare practice.
In the late 1980s, communist societies started a transition process that brought drastic changes in social values, social life, and in economic and political arrangements (Berend, 2007). In particular, the health care systems in post-communist European countries were faced with a dramatic decrease in public funding despite the significant health care infrastructure and large benefit packages established during the communist period that were preserved. Also, aside from the economic and structural changes in health care, fundamental changes in the broader social structure have occurred. In particular, collectivism with its link to wider social networks gave way to more individualistic approaches based on monetary capital with embedded personal connections (Harboe, in press). After the collapse of the Soviet Union, the state lost its de facto power in public service provision however de jure most of state's functions have remained unchanged. In order to fill the gap between regulatory and actual posture, new structures and agents – dual by nature (market and informal sector) – have emerged and have adopted some of the state functions (Williams & Onoschenko, 2014). In an overall climate of state withdrawal ‘from the provision of protection from social risks that citizens expect or need’ (Polese, Morris, Harboe, & Kovacs, 2014) in addition to public skepticism and distrust to formal institutions, individuals develop their own – ‘self-help’ or ‘do-it-yourself’ – strategies aimed at obtaining (adequate quality) services (Cohen, 2012; Mishler & Rose, 1997; Polese et al., 2014).
These changes have affected informal patient payments in the health care sector as well. During the transition period, cash informal payments started to play an important role since they facilitated the maintenance of the living standards of the health care staff who received them. Although informal patient payments are not seen as a transition feature exclusively, the prevalence of informal payments is thought to be higher in the post-communist period compared to the past (Gaal, 2004). Therefore, this paper aims to describe the magnitude and attitudes towards informal patient payments in post-Soviet and other post-communist countries. In particular, the peculiarities of informal patient payments are studied in three Eastern European countries – post-Soviet Lithuania and post-communist Poland, both members of the EU, and Ukraine: a post-Soviet non-EU country. These countries present an interesting base for a comparison with regard to differences in their socio-economic and political trajectory after communism. This paper contributes to the literature on informal patient payments with recent empirical data discussed from the angle of socio-political changes and reforms of the health care systems during two last decades. The paper is organized as follows: after the introduction, some background information on the understanding of informal patient payments and on the consequences of informal patient payments is presented. Then we outline the context of the two post-Soviet countries (Lithuania and Ukraine) and post-communist Poland, followed by the methods section which summarizes the data collection process. After that recent empirical evidence on the scope and scale of informal patient payments as well as on the public attitudes towards informal payment in Lithuania, Poland and Ukraine is presented. The final section concludes the paper by discussing the key challenges of “gifts and bribes” to health care providers in post-Soviet countries.
Informal patient payments: Understanding, prevalence and challenges
During the transition period, the terms “under-the-table”, “envelope” payments but also “bribes” or “corruption” became common labels for “gratitude” money to physicians (Kornai, 2000). The literature defines informal patient payments as cash or in-kind supplement to the official payment for health care services (Belli, 2002; Gaal, Jakab, & Shishkin, 2010) including commodities, such as pharmaceuticals and materials (Gaal, Belli, McKee, & Szocska, 2006; Lewis, 2000). A huge variety in the nature and patterns of informal patient payments is reported across countries. Previous studies have provided evidence on the variation of payment types (cash or in kind gifts given by patients or their families), timing (before, after or during service provision), subject (out- or in-patient service), purpose (obtaining better quality or access), and motivation (physician's request or patient's initiative) (Balabanova & McKee, 2002; Belli, Gotsadze, & Shahriari, 2004; Cockcroft et al., 2008; Delcheva, Balabanova, & McKee, 1997; Ensor, 2004; Falkingham, Akkazieva, & Baschieri, 2010; Gaal & McKee, 2005; Lewis, 2002; Shishkin et al., 2003; Tediosi, Aye, Ibodova, Thompson, & Wyss, 2008; Thompson & Witter, 2000). Informal patient payments include contributions to publicly-funded health care providers. Typically, the following patterns of under-the-table payments are observed: (a) expensive cash ex-ante payments paid for in-patient care, e.g. surgery or childbirth, which were expected by provider; (b) ex-post gifts in kind of a symbolic value given to out-patient care providers and initiated by the patient; (c) moderate payments initiated by the patient in order to improve health care service attributes and a variety of other combinations (Balabanova & McKee, 2002; Belli et al., 2004; Shishkin et al., 2003). Although the existence of informal payments is publicly known, the specific informal transaction takes place in secret without divulging details (Cohen, 2012). Still, the level and incidence of informal payments are difficult to compare across countries because of different methodological approaches used, as well as differences in the timing of data collection.
Seeing informal payments as purely related to culture and morality a narrow perspective. It does not fully explain the variety of informal payments. For example, payments solicited by staff do not solely reflect unethical behavior by the health care providers but also situations of chronic underfunding. Indeed consumers cannot avoid informal payments when in need of acute care.
Furthermore, country-level patient payment policies have a great impact on the scope and scale of informal payments. Indeed, informal practices are of a different magnitude and importance in countries with a similar cultural context but with distinct policies and manner of implementation. An example of a policy which has a great impact on the scale of informal payments is the official patient payment policy. Informal payments for health care services are of an unregistered and hidden nature and comprise all unofficial patient payments for publicly-funded health care services. They are examined as a type of out-of-pocket payments. However, two other types of out-of-pocket payments – formal and quasi-formal payments – refer to official patient charges for public and private health care services that may accompany informal patient payments (Belli, 2002; Thompson & Witter, 2000). In particular, formal payments are regulated by national legislation while quasi-formal payments are set by the health care provider in the absence of clear government regulations. Compared to formal and quasi-formal charges, informal patient payments claim more attention as ignoring these payments causes an underestimation of total health care expenditure and as their hidden nature imposes a great challenge to health care provision in terms of accessibility, accountability and transparency. Still, informal patient payments are not always perceived as illegal (Ensor, 2004; Gaal et al., 2006; Lewis, 2000) especially when the legislation and codes of ethics (even the moral codes) in the country do not prescribe proper conduct and behavior.
Also, regulation and monitoring of gift-accepting or gift-denying behavior of providers may strengthen professionalism and therefore make service provision more transparent. Studies show that informal patient payments are not unique to post-Soviet and post-communist countries. They are a well-known phenomenon around the world. The practice of small gifts (flowers, chocolates, wine) given by the thankful patient to health care staff after service provision exists in many countries (Abbasi & Gadit, 2008; Barr, 1996; Chiu, Smith, Morlock, & Wissow, 2007; Lyckholm, 1998). Such gifts are not typically expected by providers and the amount and quality of the treatment patients receive is not dependent on it. Although it is recognized that such gifts should be regulated and monitored, they are not seen as a problem in health care provision (Dodge, 1978; Greenberg, 1990; Orentlicher, 1994) as long as patients who do not give gifts, are not deprived from adequate health care services. Rubin (2012) even argues that such small gifts to physicians should not be forbidden since gift refusal may hurt the feelings of the patient. Therefore, in exceptional cases, medical professionals have asserted their right to accept small gifts from patients. Still, these exceptional cases of informal exchanges between patient and medical doctor exist in the context of strong norms and regulations which shape staff behavior.
Overall, the boundaries between forms of informal payments – between true gifts that are perceived positively and solicited payments which have negative and harmful connotation, e.g. bribes – are blurred (Polese, 2008; Wanner, 2006). In contrast to other services (e.g. hairdresser), health care service users are usually less informed about the care that they need and the costs associated with it. In the case of no formal patient charges, there is no agreed price-list and it is rare that a payment is directly requested by the physician. The context in which informal payments occur is rather ambiguous. Patients are typically aware of the possibility or need to pay to the physician but unlike the physicians, patients are usually inexperienced in ‘ensuring adequate service provision’ through informal payments. Indeed, informal payments are conducted in a trustful relation, in a specific atmosphere. The ability to recognize a hint or a good moment for payment is desirable to achieve a satisfactory result.
Meanwhile, there are more elements that facilitate a division of the wheat from the chaff. Specific local norms typically define which types of exchanges can be treated as corruption. However, for post-Soviet countries, corruption is a relatively new concept (Rose-Ackerman, 2010) which supplemented a list of well-known phenomena, i.e. bribery, patronage and pilferage (Werner, 2000). Meanwhile, discussions about variations in the meaning and interpretations of corruption are highly relevant when the ranking of countries with different connotation of corruption, is on the agenda. A negative connotation of corruption is mostly indisputable, and perceptions of informal ‘fee-for-service’ or donations to health care providers as corruption can vary greatly between years and countries. In practice, physicians continue to provide health care services and are involved in routine exchanges of fees, gifts, and cash given by patient. This type of exchange is often euphemistically called ‘gift giving’. However, these payments have little in common with real gifts. When anti-corruption legislation is strictly enforced as well as the punishment of corruptive actions is a real risk for parties involved, the connotation of ‘corruption’ shifts to socially undesirable behavior. As a result, the borders between gifts and bribes become more apparent and informal payments are likely to diminish. When candid bribes are not prosecuted, general moral dispositions in society such as “everything that is not forbidden is allowed” may well predispose wide-spread cash informal payments and corruption in the health care sector.
However, the important issue is the dimension of the (non)conditioned provision of health care services. The physician may be reluctant to provide detailed information about the diagnosis and treatment, or may avoid referring the patient to the most suitable specialist, or even ignore the patient if no informal payment is offered (Allin, Davaki, & Mossialos, 2006; Cohen, 2012; Ensor & Witter, 2001; Gaal et al., 2006; Lewis, 2002, 2007; Pavlova et al., 2010). Consequently, informal payments may affect the physician's decision on what services to provide and to whom to provide them. Parallel to the informal payment however, physicians or health care facilities also receive a formal reimbursement (public funds) for services provided. Thus, although at first sight both providers and informal payers benefit from the informal exchange, the allocation of public resources is also affected by the individual's willingness to pay informally, not just the social value of the use of these resources. In view of this, informal payments are seen as providing incentives to physicians. If there are patients willing to receive and willing to pay informally for less cost-effective services, then the cost-effectiveness of health care service provision is also undermined. In view of this, informal patient payments can become a major impediment for health care delivery and reforms that aim at the efficient use of public health care resources.
Although informal payments may help individual patients to obtain services with better quality (Mæstad & Mwisongo, 2011; Thompson & Xavier, 2004), there is no evidence that these payments significantly contribute to the improvement of clinical quality in the health care sector in general (Gaal & McKee, 2005). Empirically tested (e.g. quasi-experimental) findings that support or refute the impact of informal payments on the attributes of services provided (including quality attributes) are lacking. It is recognized that health care providers are not interested in reinvesting the informal payments in the public health care system (e.g. purchasing new medical equipment) but are more likely to invest them in their own private practice or use them to supplement their income (Belli et al., 2004; Gaal et al., 2006; Kornai, 2000; Mæstad & Mwisongo, 2011). In the long-run, this may lead to better quality of services provided in the private sector (for those who can afford to pay the fees) than in the public sector, even if provided by the same physician. The most negative effects of informal patient payments are noted when patients who lack funds or social protections, and cannot afford to pay informally, either avoid or delay seeking treatment (Lewis, 2007). Frequently, they use personal savings, take out loans and sell assets to cover these payments. The ultimate effect is the same as referring patients to the private health care sector. In some instances, low-income patients are found to pay informally proportionally more in relation to their income than high-income groups. In fact, informal patient payments are highly regressive even when compared to formal co-payments (Baji, Pavlova, Gulácsi, & Groot, 2012; Mastilica & Božikov, 1999; Özgen, Sahin, Belli, Tatar, & Berman, 2010). The idea that physicians (guided by a “Robin Hood” principle) charge rich patients informally and provide free-of-charge service to poor patients (Morris & Polese, 2014; Stan, 2012) is not supported by empirical quantitative findings (Szende & Culyer, 2006).
Therefore, a variety of interrelated factors which are associated with informal payments are tackled by different authors (Gaal & McKee, 2005; Thompson & Witter, 2000; Tomini & Maarse, 2011) who argue that the presence of informal patient payments can be explained by the tradition of giving gifts as mentioned above, as well as by other cultural, social and ethical factors that do not directly affect the health care system. Overall, four basic dimensions are noted in the literature (Gaal & McKee, 2005; Mossialos et al., 2002; Tambor, Pavlova, Woch, & Groot, 2011; Tomini, Groot, & Pavlova, 2012) – socio-cultural factors, economic and labor factors, political and regulatory factors, and health care systems in particular – that can be used to classify the factors and shed a light on the causes of informal payments. It should be pointed out however that the dimensions (factors) are rather interwoven leading jointly to the existence of a specific pattern of informal payments in a country. For example, the existence of informal payments is associated with insufficient health care system funding and low physicians’ salaries (health care system dimension). This offers an explanation of why health care providers request informal payments and emphasizes the providers’ role in the informal payment chain. Nevertheless, insufficient health care sector funding is largely a result of poor economic circumstances (economic and labor dimension), which in turn limit the resources available for public health care provision. Thus, the two dimensions, the health care sector and the economic and labor environment, are interrelated and it might be difficult to distinguish their intertwined influence in practice.
Similarly, the socio-cultural factors indicate the role of society but also the role of the patient as a key element of the informal payment chain (health care system dimension). Thus, even when the informal payment is requested, the patient makes the final decision to resort to an informal transaction with the provider or not. In other words, the patient is able to pour oil in the flame of the defective regulatory mechanisms and the economic climate that leads to informal payments. But it is also the patient who initiates informal payments as a means to obtain the desired services. Cohen (2012) describes this behavior as a “do-it-yourself” approach – an adaptive strategy of an individual who is unsatisfied with government services and is willing to apply different (e.g. informal or “extra-legal”) approaches to fulfill health care needs. Therefore, theoretical discussions (Gaal & McKee, 2004) and empirically tested theories (Burak & Vian, 2007) offer a deeper look at individual motives for informal payments.
The culture of giving gifts seems to be the most straightforward explanation that applies beyond the borders of a single country. However, in the context of inadequately funded public health care services, informal payments also provide a means for patients in post-communist and post-Soviet European countries to receive services with quicker access and better quality, as well as to health care providers to obtain adequate reimbursement for services provided (Belli, 2002; Chawla, Berman, & Kawiorska, 1998; Cockcroft et al., 2008; Tatar, Özgen, Sahin, Belli, & Berman, 2007).
Given the above, a better understanding of the country-specific context is essential for a full picture of informal patient payments.
Health care systems and the socio-political context of post-Soviet and post-communist European countries
The transition from a state-planned to a market economy has created a mix of contrasting political and social values, and a continuously changing socio-economic environment in post-communist countries (Deppe & Oreskovic, 1996). There are also other disadvantageous trends (poor health indicators, unemployment, low salaries of medical staff, lack of trust). The cases used in this analysis – Lithuania, Ukraine and Poland – have a lot in common, though they also show some diversity in terms of economic development, demographic patterns, and health indicators and also, the extent of the problematic areas differs between the countries. The characteristic features of these three countries are briefly described in this section.
The economic development of the countries is tightly related to the fiscal revenues allocated to the “non-profit” sectors. Insufficient resources are often attributed to the incapability of the government to ensure an adequate level of public services provision. Indeed, two decades ago, virtually all post-communist European countries experienced an economic recession and difficulties in revenue collection also in the health care sector. Later, the majority of the countries in the region experienced economic growth, especially those who joined the EU (e.g. Lithuania and Poland) but not the countries from the Community of Independent States (e.g. Ukraine) due to the slow privatization process, the widespread corruption and the distance from European markets.
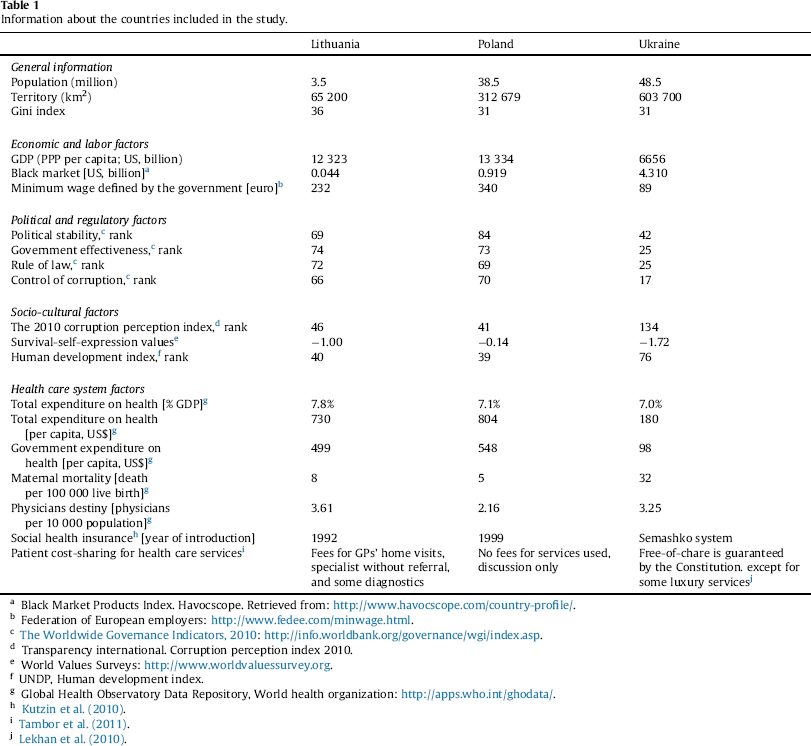
Generally, a shortage of resources as well as a lack of good governance is characteristic of all post-Soviet countries (Gaal, 2004; Kuszewski & Gericke, 2005; Lekhan, Rudiy, & Richardson, 2010). Less developed countries spend less on health care per capita and rely on public funds, whose share varies widely (from 40 to 85%) (WHO, 2013). As presented in Table 1, Lithuania, Poland and Ukraine spend a similar share of GDP on health care (about 7–8%). However, the expenditures on health care per capita differ: US$730, 804 and 180 respectively, as well as the government expenditure on health care per capita: US$ 499, 548 and 98 respectively.
Information about the countries included in the study.
Information about the countries included in the study.
Black Market Products Index. Havocscope. Retrieved from: http://www.havocscope.com/country-profile/.
Federation of European employers: http://www.fedee.com/minwage.html.
The Worldwide Governance Indicators, 2010: http://info.worldbank.org/governance/wgi/index.asp.
Transparency international. Corruption perception index 2010.
World Values Surveys: http://www.worldvaluessurvey.org.
UNDP, Human development index.
Global Health Observatory Data Repository, World health organization: http://apps.who.int/ghodata/.
Kutzin et al. (2010).
Tambor et al. (2011).
Lekhan et al. (2010).
The availability of resources matters, but also its management. The quality of governance can be measured by such indicators as the rule of law, government effectiveness, political stability and others. By and large, the scores of Poland and Lithuania are higher than the Ukrainian; however they are lower than the scores of Western European countries (The Worldwide Governance Indicators, 2010).
Considering the experience of the post-communist countries, Poland has one of the best governance indicators in the region (The Worldwide Governance Indicators, 2010), presenting a case of a “season of corruption” in contrast to the deep-rooted “climate of corruption” in other post-communist countries (Miller, Grødeland, & Koshechkina, 2001). Poland provides an example of the implementation of anti-corruption measures (realized in cooperation between related sectors) (Golinowska, 2010). Only after such institutional anti-corruption measures are put in place with a special focus on informal patient payments, have mass-media been engaged in Poland. Possibly, anti-communist public moods, a lack of nostalgia as well as the intention to join the EU facilitated the reforms in virtually all sectors (Leven, 2005). Thus, quality of governance is crucial to diminish the extent of informal patient payments and of the informal sector in general.
The capacity of the government has been also reflected in the depth of the health care reforms in the countries. More than one decade ago, almost all Eastern European countries, including Lithuania and Poland but not Ukraine, switched from a system of central planning and free-of-charge health care to a decentralized system with a health insurance fund. While Ukraine largely preserved the tax-based health care system established during communism, Lithuania and Poland already established a social health insurance system in the 1990s. In Lithuania, access to health care is assured for the vast majority of residents while the working population is obliged to join the state health insurance scheme and the state increasingly contributes for non-economically active inhabitants presenting over 60 percent of the total population (Murauskiene, Janoniene, Veniute, van Ginneken, & Karanikolos, 2013). In Poland, social health insurance covers about 98% of the population with a comprehensive benefit package (Golinowska & Tambor, 2012; Sagan et al., 2011).
Also, Lithuania and Poland have achieved more in the field of reducing hospital capacity and extending primary health care (GPs play a gate-keeping role and are paid per capita), as well as in improving quality and equity in health care provision and the cost-effectiveness of health care provision (Murauskiene et al., 2013; Sagan et al., 2011).
The systems of patient payments for health care services are considered to be unclear in Ukraine where the Constitution guarantees free-of-charge health care services and a list of luxury “paid services” has been introduced. In Lithuania, payment regulations seem to be more grounded. Lithuanians who are non-residents, non-insured, non-registered by GP are charged for using non-vital health care services (Murauskiene, Pavlova, Veniute, & Groot, 2012; Murauskiene, Veniute, & Pavlova, 2010). In addition, a price-list has been developed in case of consumption of services from the negative list of (mostly auxiliary) services. Quasi-formal payments and informal patient payment are considered to be widespread but they are not subject of consistent policy debates and are not always recognized by policy-makers as essentially problematic. Recently, the Lithuanian government has attempted to regulate the quasi-formal payments that had been introduced by public health care facilities. Meanwhile, in Poland, discussions on the possible introduction of patient payments have taken place, which has not resulted in new policies (Tambor et al., 2011).
It is important to underline the features of the socio-political environment of Lithuania and Poland (additional to those presented in Table 1), which joined the EU in 2004. EU membership provided a framework and stimulus to improve regulations, to achieve better living standards, more transparency and accountability. It also required the eradication of corruption. Meanwhile, Ukraine is a non-EU member and until recently had doubtful chances to achieve this membership.
The countries experienced numerous appointments of ministers of health during the last decade (e.g. 8 in Lithuania, 10 in Ukraine and 13 in Poland with an average length of stay of 1–1.5 year). The general political and social situation has also not been very stable in the countries during the past years. Wanner's suggestion that the “Europeanness of Ukraine is more questioned than that of the Baltic or other former-socialist Eastern European countries” (2006: 517), is also confirmed by the EU-membership of Lithuania and Poland in contrast to Ukraine. However, in these countries, political and economic changes have also entailed new combinations of individual-social interests (more orientated to individual ones) as well as new consumer values. However, during transition, post-Soviet societies lost trust in authorities due to the loss of principles of social welfare (Dobryninas, 2005; Polese, 2008; Polese et al., 2014; Wanner, 2006). In particular, the overall situation in Ukraine before the revolution in 2014 was characterized by a monopolization of political and economic power by political forces for self-enrichment as well as by the lack of public trust in state institutions coupled with non-fulfillment of political and economic obligations (Kuzio, 2012). At the same time, Lithuania endures a demographic crisis, i.e. negative population increase and one of the highest emigration rates in Europe.
Summarizing, the environment in Ukraine is relatively more conductive to informal payments compared to that in Lithuania and especially in Poland with regard to differences in economic, regulatory and health care system, and perhaps to a lesser extent differences in the cultural environment in the countries.
In July 2010, nationally representative identical household surveys were conducted in Lithuania, Poland and Ukraine. 1000 completed interviews were collected in each country. A stratified random sample was drawn in three countries following a multi-staged random probability method. Firstly, the sampling points in each country (ca. 150 sampling points per country) were distributed proportionally to regional, urban/rural and ethnic characteristics of the population. Secondly, 8–10 addresses/households per sampling point and thirdly, one adult member (older than 18 years) per household were selected for interview. If the respondent determined on stage 3 refused or was unavailable to take part in an interview after two call backs, a replacing respondent was identified following stage 2–3.
The mode of data collection was face-to-face interviews based on a standardized questionnaire. The research instrument was developed in English and then translated. The translation was verified using the method of backward translation by an independent translation agency to check preservation of meaning. The questionnaire was kept identical for countries to ensure a meaningful comparison of the results between the countries. Prior to the survey, the interviewers were trained to clarify the fieldwork standards and the specificities of the questionnaire. A high number of interviewers were involved in the surveys to avoid interviewer bias.
All respondents were asked about their attitude toward informal cash payment and gifts in kind and whether they associate cash or in-kind gifts with corruption. In these questions, cash payments and in-kind gifts were separated since the perception of gifts was expected to be dissimilar to that of cash payments. Respondents could agree or disagree with the statements about the inevitability of informal payments because of low health care funding and about the need of eradicating informal patient payments. Additionally, interviewees were also asked to confirm, deny, or express ambiguity about five perception statements that indicate individual acceptance or readiness to pay informally for health care (e.g. being unable to refuse to pay informally if asked). Also, we asked respondents about their past experience with informal payments and related total expenditures as well as informal part of it (the overall monetary estimation of the gifts in kind and cash given for the service). In this question, public and private services are not divided to account for differences in the system of health care service provision. Except for the abovementioned questions on informal patient payments analyzed here, the questionnaire included other parts focused on preferences for health care services and also a socio-demographic section. On average each interview lasted 30 min.
The patterns and attitudes towards informal payments in Lithuania, Poland and Ukraine
Data on the scope and level of informal patient payments in post-Soviet Lithuania and Ukraine, and post-communist Poland suggest widespread informal practices in health care provision in Ukraine, to a lesser extent in Lithuania and much lesser extent in Poland. In particular, there is a variety of differences in the organization and financing health care service provision as well as a mixture of patient payment policies in the countries that accompany informal payments.
The scope and level of informal patient payments
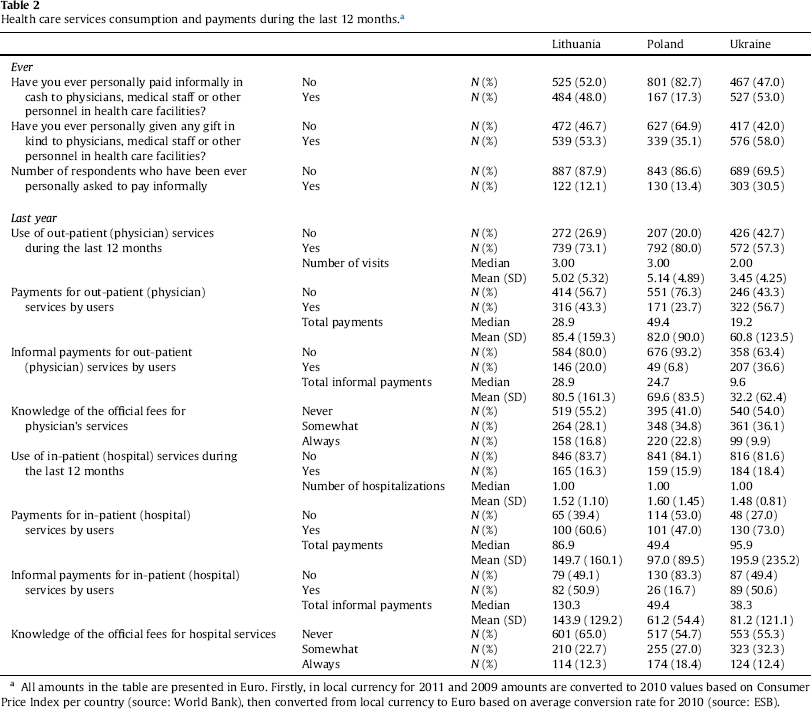
Table 2 shows the valid percentage of respondents and the number of those who report that they have ever paid informally in cash or in the form of in-kind gifts. In Lithuania and Ukraine, the percentage of those who have ever given cash to medical staff is almost the same (48% and 53% respectively) in contrast to 17% reported by Polish respondents. A higher percentage of respondents report that they have ever made informal payments to medical staff in the form of in kind gifts compared to cash payments. Moreover, each third respondent in the Ukrainian sample in contrast to each eight respondent in the Lithuanian and Polish samples has ever been asked to pay informally for health care services. Similar results are reported in Lithuania and Poland in a recent study (Study on Corruption in the Healthcare Sector, 2013). Generally, informal payments are more widespread when they are solicited or expected by providers, and also higher amounts of informal payments are given at the medical staff's request as suggested by previous studies (e.g. Tomini et al., 2012). According to Cohen (2012), solicited informal payments can be seen as an indicator of major financial troubles in the health care system, while patient-initiated informal payments can be related to unmet patients’ expectations of better service quality.
Health care services consumption and payments during the last 12 months.a
Health care services consumption and payments during the last 12 months.a
All amounts in the table are presented in Euro. Firstly, in local currency for 2011 and 2009 amounts are converted to 2010 values based on Consumer Price Index per country (source: World Bank), then converted from local currency to Euro based on average conversion rate for 2010 (source: ESB).
Furthermore, the probability and the size of the informal payment is to a great extent determined by the type of service consumed (out-patient or in-patient care). The results presented in Table 2 suggest a higher number of users and amounts that are paid for hospitalizations. The literature also provides evidence on more expensive payments paid by a higher share of patients during a hospitalization (Kornai, 2000; Shahriari, Belli, & Lewis, 2001; Szende & Culyer, 2006; Tomini & Maarse, 2011; Vian, Grybosk, Sinoimeri, & Hall, 2006). In detail, when the annual proportion of informal payers is examined it appears that about 7% of Poles, 20% of Lithuanian and 37% of Ukrainian out-patients, and about half of the in-patients in Lithuania and Ukraine in contrast to 17% in Poland, pay informally. Ukrainians report a median value of about 15 Euro in informal payments per respondent per year while this is about 44 Euro in Lithuania and Poland. When the means of the informal patient payments per respondent per year are compared with the minimum wage in the countries (see Eurostat, 2010), it appears to be virtually equal to one monthly minimum wage in Ukraine, to half of it in Lithuania and to quarter in Poland. Taking into account the share of those who are unable to pay (Tambor et al., 2014), this indicates a considerable burden on households caused by informal patient payments (especially for lower-income households and especially in Ukraine).
It is worth mentioning that informal patient payments can co-exist with other types of patient payments such as quasi-formal and official patient payments. When a clear regulation of the basic package and formal patient charges is lacking, patients experience a mixture of payment obligations. For example, we observe that informal payments are a wide-spread supplement to also widespread quasi-formal payments in Lithuania and Ukraine. Meanwhile, patients in these two post-Soviet countries are poorly informed about the size of the formal fees as indicated in Table 2. Therefore, similar practices of informal payments constitute a behavioral pattern in health care consumption. Perhaps, a common social past provides a lot of similarities however more modest nature of the phenomenon in Lithuania can be stipulated by higher levels of economic development and governance practice.
Public opinion, though infrequently considered in policy making, can play an essential role in dealing with informal payments (Ensor, 2004). Culture, social norms and historical developments in a country influence individual attitudes and behavior (Gatti, Paternostro, & Rigolini, 2003). Public acceptance enables the existence of payments and may hinder elimination. Moreover, public opinion towards a social phenomenon (such as informal payments for health care) may affect behavior of individual patients and providers, and thus, the specific patient–provider relation where informal payments originate from.
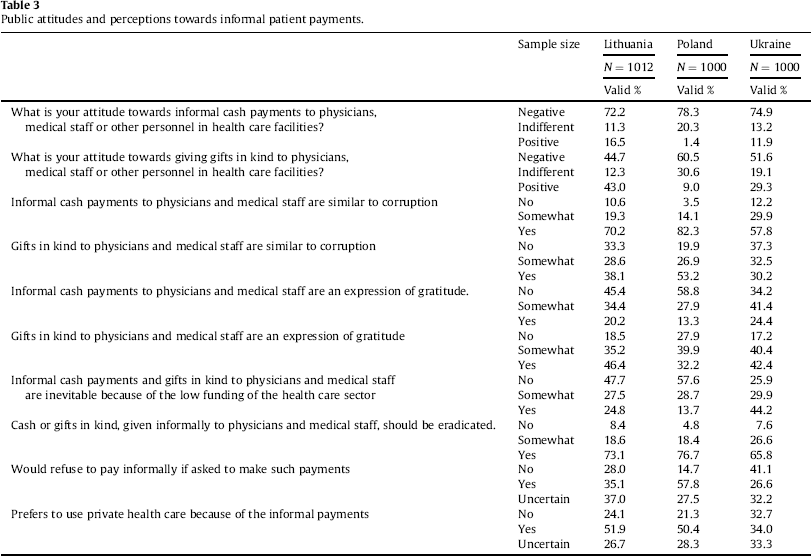
Therefore, recent data on public attitudes and opinions are highly important. Table 3 shows the valid percentage of respondents per country, who stated their perceptions and attitudes toward informal patient payments. Generally, the attitude towards informal cash payments and to a lesser extent towards in-kind gifts is overall negative among the public in Lithuania and Ukraine and even more in Poland. The attitudes towards cash informal patient payments are rather negative (72% in Lithuania, 75% in Ukraine and 78% in Poland) whereas a relatively lower percentage of people in Lithuania, Ukraine and Poland (45%, 52% and 61% respectively) report negative attitudes and are not afraid to voice a positive attitude towards in-kind gifts.
Public attitudes and perceptions towards informal patient payments.
Public attitudes and perceptions towards informal patient payments.
Previous studies have also reported on the prevalence of negative attitudes towards informal payments as well as a more positive attitude to in-kind gifts compared to cash payments (Balabanova & McKee, 2002; Belli et al., 2004; Cockcroft et al., 2008; Tatar et al., 2007). Although in-kind gifts (as well as cash payments) can be considered as a means to obtain better and quicker services when the system fails to offer adequate service standards to all patients, in-kind gifts are not supposed to induce expenditures beyond the patient's means. Tokens of gratitude are common practice all over the world but the extent of the gift-giving practice might differ (Abbasi & Gadit, 2008; Spence, 2005) as in some countries clear regulations of physician behavior are more developed and adhered to (Gaufberg, 2007; Kutzin, Cashin, & Jakab, 2010; Rechel, Blackburn, Spencer, & Rechel, 2011). Moreover, when gifts are not expected and encouraged, they do not adversely affect efficiency in health care provision (Gaal & McKee, 2005).
Another dimension of consumers’ acceptance of informal transaction is to label it as “corruption” or “gratuity”. As is shown in Table 3, there is widespread adherence to the notion that informal cash payments are similar to corruption and that in-kind gifts are an expression of gratitude. Still, diversity of opinions is observed in midpoints, for example, about 20–24% of the public in both Lithuania and Ukraine and about 13% in Poland believe that informal cash payment can be seen as gratitude. Also, 30% of respondents in Ukraine, 38% in Lithuania and higher portion in Poland (53%) think that in-kind gifts given to medical staff can be treated as corruption.
As public attitude can typically be seen as public moods translated via media, it is also important to have a deeper look at individual consumers’ perceptions. Specifically, disposition (attitudes coupled with previous experience) is a personal construction that ensures specific behavior to occur in a given situation and is seen as a regulatory mechanism of human behavior (Uznadze, 1966). However, it is difficult to measure, especially in cases of informal patient payments. Therefore, we attempt to examine perceived behavioral statements related to informal payments (that indicate personal disposition towards these payments). As a result, we observe that those who feel uncomfortable without giving a gratitude payment and who feel unable to refuse to pay informally if asked, more often report making informal payments than the rest of the respondents.
As it is shown in Table 3, 33% of Ukrainians and 21–24% of Poles and Lithuanians have chosen the “no” answer on preferences for paying officially in the private health care sector instead of making informal payments in the public one. Also, on the question “would you refuse to pay informally if asked to make such payments” fewer Lithuanians and even fewer Poles answer negatively in contrast to Ukrainians when asked (28% and 15% in contrast to 41% respectively). Perhaps differences in patterns of patient–physician communication with more empowered Lithuanian and Polish patients may explain the diversity in the scores as well as consequences of such refusal. Overall, the obedience to the requests of medical staff to pay informally can be conditioned by patients’ expectations for better treatment or by a fear that treatment can be denied (Belli et al., 2004; Lekhan, Rudiy, & Shishkin, 2007). The latter is explained by the market power of health care providers as well as by external pressure (Jancsics, in press), e.g. by low-paid medical staff, who in the absence of free patient choice, bring informal practices to the patient–physician relation (Aarva, Ilchenko, Gorobets, & Rogacheva, 2009; Miller, 2006). This also may indicate variations in cultural context in these countries. Still, as data are lacking, it is difficult to track the changes of consumers’ disposition with regard to economic, legislative and health care sector development.
The key challenges in the eradication of informal payments become more visible when the scope of and attitudes towards informal payments are considered in the light of economics and governance. In Lithuania, Poland and even more in Ukraine, it is possible that the public is willing to change their pattern of behavior but poor governance, economic development and low health care funding leave much to be desired.
A key function of informal payment in services provision is seen in supplementing inadequate health care funding (Lewis, 2007). Indeed, in Lithuania, Poland and in Ukraine, per capita government expenditures on health care is even lower than in other countries in the region where informal payments are negligible, namely the Czech Republic and Slovenia (Leive, 2010; WHO, 2010). In addition, our survey results indicate that about 14% of Polish and 25% of Lithuanian respondents consider informal payments for health care to be inevitable because of the low health care funding whereas this percentage is even higher for Ukraine (44%). Furthermore, the Lithuanian, Polish and Ukrainian public support the statement that informal patient payments should be eradicated; only about 5–8% are sure that this is not necessary.
Low funding of the public sector affects preeminently public service providers’ official salaries. Since the 1950s, the communist ideology promoted community interests rather than individual enrichment (Gaal & McKee, 2005). Thus low wages of physicians were politically stipulated. However, after the Soviet Union the tradition of low-paid health care staff has not changed, leading to a popular ‘poorly-paid doctors’ excuse for resorting to informal payments. Granovetter (2007, p. 155) suggests that “employers knowingly pay lower wages than they or the employee think reasonable, assuming that some pilferage will take place that makes up the difference”. Moreover, in some instances, physicians are found to earn as much as a full additional salary from informal payments (Baji, Pavlova, Gulácsi, & Groot, 2011; Betliy, Kuziakiv, & Onishchenko, 2007; Ensor & Savelyeva, 1998; Falkingham, 2004; Kornai, 2000). Still, certain specialties like surgery, gynecology and dentistry allow earning higher informal remunerations compared to others leading to an unequal distribution of income and therefore, creating inadequate work conditions for unattractive specialties.
Conclusions
The empirical results show that informal payments are often used in health care services. Patients resort to making informal payments, but at the same time public opinion on informal payments for health care is negative. The problem of informal payment is complex and relates to the imbalance between actual provision and services expected. Therefore, the dominant ‘culture’ of gift-giving or donations in health care can be seen not as a voluntary practice but rather as forced actions in terms of the failure of social welfare provision (Davies & Polese, in press). Also, important details of the organization and financing of health care service delivery may contribute to our understanding which features of health care system force patients to specific actions that consequently form a unique pattern of informal patient payments in the country.
The low level of salary of health care personnel is typically considered as the most important factor that explains the spread of informal patient payments (Belli, 2001; Healy & McKee, 1997; Rechel & McKee, 2009; Van Lerberghe, Conceição, Van Damme, & Ferrinho, 2002). Lower physicians’ salaries compared to the country average or to the industrial sector average provide a motive for patients and physicians to go into informal payment arrangements. A quotation of Mauro (1997) presented by Shahriari et al. (2001) underlines a basic principle of underpaid public service providers to rely on informal revenues: “When civil service pay is too low, civil servants may be obliged to use their positions to collect bribes as a way to make ends meet.” However, the increase of health care staff remuneration will not be a panacea for the problem of informal patient payments. For example, in Lithuania health care providers’ salaries were increased in 2005–2008 but informal patient payments still prevail (Murauskiene et al., 2013). Except for the level of salary in the health care sector, a performance-based provider payment mechanism may play an important role in stimulating the provision of sufficient quality and quantity of services. Similar to Western European countries, some post-communist countries have introduced per capita payment systems for GPs (e.g. Poland and Lithuania as it is mentioned above). In Ukraine, the newly established practice of family doctors involves this practice but is limited to a number of pilot regions. Chawla, Tomasik, Kulis, Windak, and Rogers (1999) indicates that only the capitated primary care physicians did not charge additionally, namely, those physicians whose earnings were highest due to the adequacy of the per capita payment and the patterns of demand. However, in-patient personnel are usually paid salaries (Groenewegen, Dixon, & Boerma, 2002; Kutzin et al., 2010).
Still, political and economic changes in the Eastern European countries (especially those related to public services provision, given its degree of accountability and transparency) are seen as key determinants to informal exchanges flourishing. Informal payments serve as a means for individuals to achieve at least a higher individual welfare when the state fails to ensure social welfare (Wanner, 2006). Consequently, underpaid health care staff is one of the many other failures of government policy. Particularly, when quality standards (protocols) are absent or when their application is not monitored, in a context of underfunding, providers themselves may choose the attributes of the service to be offered to the patient. Thus, in order to have control over the quality of care, patients resort to informal payments which are perceived as a tool of control (Stan, 2012). However, patients are not able to recognize divergences in terms of clinical quality unlike service wrapping. Furthermore, in the context of service quality ambiguity, erosion of trust erodes the patient–provider relation, which has consequences for treatment outcomes as well. A similar effect is observed in case of a negative attitude of medical staff to patients. Taking into account the market power of health care providers as well as the issue of information asymmetry, patients appear in a vulnerable position that has also been suggested by our empirical results on consumers’ perceptions.
Also, outdated equipment and improper state of facilities become barriers for adequate service quality. The lack of suitable investments is seen as a direct result of underfunding but also of an inefficient management of health care resources. Informal patient payments as well as quasi-formal payment may well fill gaps in funding of health care facilities (Gaal et al., 2010; Lewis, 2000). A recent study on how resources of health care facilities are managed in Ukraine provides evidence that informal payments given by patients to medical doctors can be re-invested in practice and in facility maintenance: individual health care providers buy bulbs, detergents as well as pay for their professional growth, including trainings, etc (World Bank, 2014).
Informal payments (e.g. for health care services) are more deeply rooted in the countries where the government tolerates and relies on informal payments since these payments are an additional source of funding. Therefore, informal payments – which have existed for decades as an acceptable practice – shift from deviant behavior to a normative one bringing a mismatch in the health care sector goals and in the measures applied to achieve the goals. The privatization of health care takes place de facto. At the same time, the public seems to be unsatisfied with how public services are provided. Although the presence of a civil society is a political regime attribute, public interests can be represented via a civil society that can influence the level of corruption (Grimes, 2008), or can play the role of “anti-corruption watchdog” (Grødeland & Aasland, 2011). Still, policy-making in most post-communist countries (including post-soviet countries) frequently serves the interests of top-business (e.g. Kuzio, 2012). The medical elite is not interested in reforms aimed to harmonize responsibly and redeem patients from financial burden (Gaal & McKee, 2005). The problem is not only in informal payments but also in the transformation of health care system as a whole.
Acknowledgment
The study is financed by the European Commission under FP7 Theme 8 Socio-economic Sciences and Humanities, Project ASSPRO CEE 2007 (GA no. 217431). The content of the publication is the sole responsibility of the authors and it in no way represents the views of the Commission or its services.