
Abstract

In the optimistic environment of an expanding economy and population, the newest medical school in Canada was established in 1967 at McMaster University, Hamilton, Ontario. In response to newer understanding of adult education and also reflecting dissatisfaction with traditional approaches to medical education, this new medical school had no formal lectures, embedded its teaching philosophy in problem-based learning and established a process of continuous evaluation of students with no written examinations. In approximately 30 years the medical school has established and enhanced a strong international reputation in teaching and research. A new teaching hospital, McMaster University Medical Centre (Chedoke-McMaster Hospitals) was built for the medical school and the 3 existing hospitals, the Hamilton General, Henderson General and St. Joseph's Hospital, became partners with McMaster University through affiliation agreements.
Each of these hospitals had its own integrated Department of Laboratory Medicine with the relatively traditional disciplines of Clinical Chemistry, Hematology/Transfusion Medicine, Microbiology and Anatomic Pathology/Cytology. However, in partnership with McMaster University Department of Pathology, the four hospital Departments of Laboratory Medicine cooperated in a Hamilton Regional Program to ensure a rational use of laboratory resources and an optimal distribution of academic services.
Over 25 years this allowed the development of an efficient and innovative program with a tradition of cooperation and trust.
THE CANADIAN HEALTH CARE SYSTEM
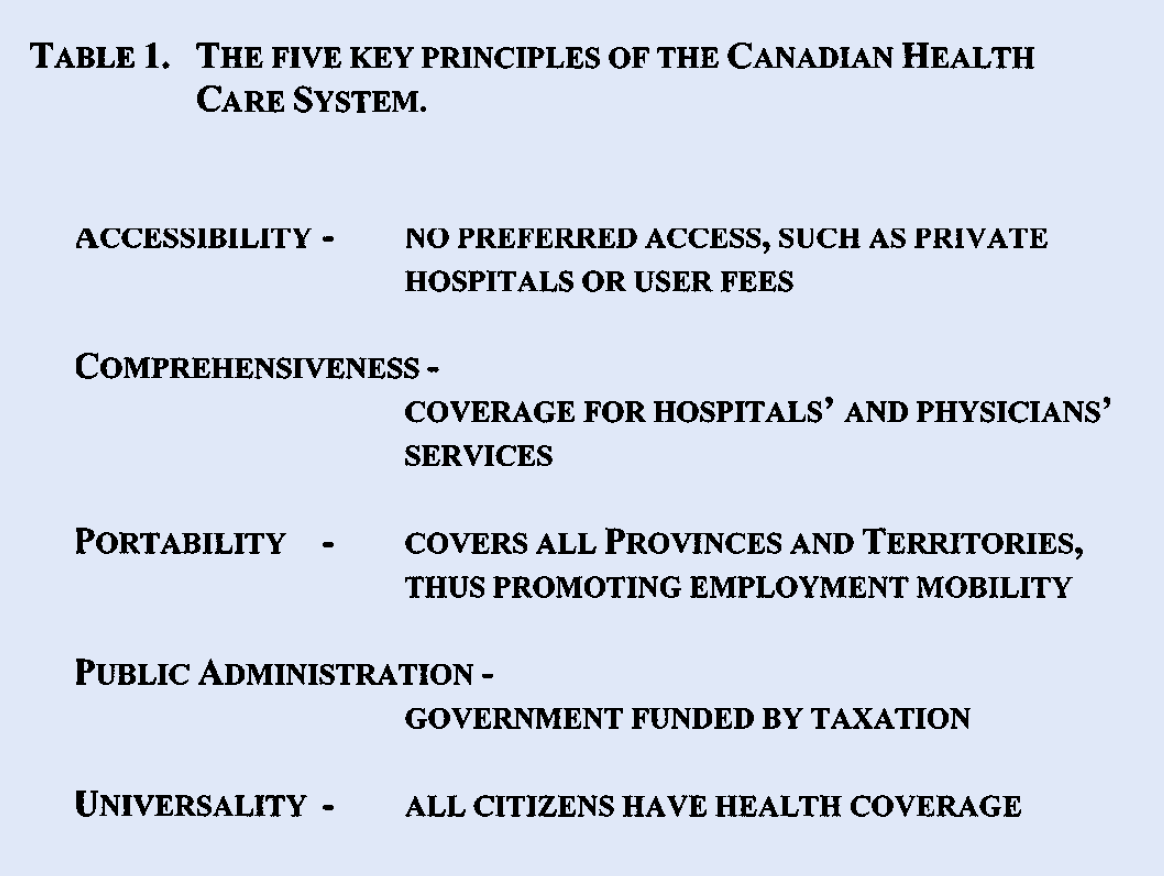
The public health system in Canada, Medicare, is based on five principles (
THE FIVE KEY PRINCIPLES OF THE CANADIAN HEALTH CARE SYSTEM.
LABORATORY COSTS AND REORGANIZATION IN THE PROVINCE OF ONTARIO
Ontario has approximately 11 million people, representing about one-third of the population of Canada. In 1998–1999 the hospital and private laboratory services in Ontario each received approximately $500 million (US $325 million) from the Ontario Ministry of Health, in total representing 5% of the Provincial health expenditure. About 35% of the Provincial Government annual revenues are spent on health care in Ontario. Reduction in expenditure of laboratory services is part of the health care reform plans in the province. Some laboratories have been closed, others have been reduced in size. The hospital and private laboratories have been encouraged to form strategic alliances to improve accessibility, maintain quality, the classic expectation of “doing more with less”. Many hospital administrators fail to understand the vital role of the laboratory in prevention, diagnosis, prognosis and management of illness.
The laboratory has been viewed as a support service rather than a clinical service.(6) Reductions in the laboratory budgets have been seen as a revenue source for other services. In addition, highly paid external consultants have been engaged to impose solutions. These tend to be financially dominated and show little sensitivity for the teaching and research responsibilities of academic departments of laboratory medicine. It is difficult to get exact figures but it has been estimated that approximately $150,000,000 has been removed from Ontario hospital laboratory budgets since 1992. In March of 1998 the Ontario Government tried to prevent further erosion of laboratory services by freezing the hospital laboratory budgets. However, much of the damage was already done and there is a lack of evidence that this directive has been followed by many hospital administrators.
THE IMPACT OF DOWNSIZING ON SERVICE AND ACADEMIC ACTIVITIES
When experienced and knowledgeable staff are laid-off or given early retirement there is a loss of analytical and management expertise. There is already a shortfall in the numbers of Laboratory Physicians and Scientists and further reductions exacerbate this problem. Fewer experienced senior laboratory technologists has a significant impact on the quality of service being delivered. Promotion of new managers with less experience or insight into the demands of laboratory services reduces the efficiency and effectiveness of the laboratory operations. Quality, education, service and research all suffer when all levels of staff are overworked and many are relatively less experienced.
IMPACT ON MEDICAL LABORATORY TECHNOLOGISTS, LABORATORY PHYSICIANS AND SCIENTISTS
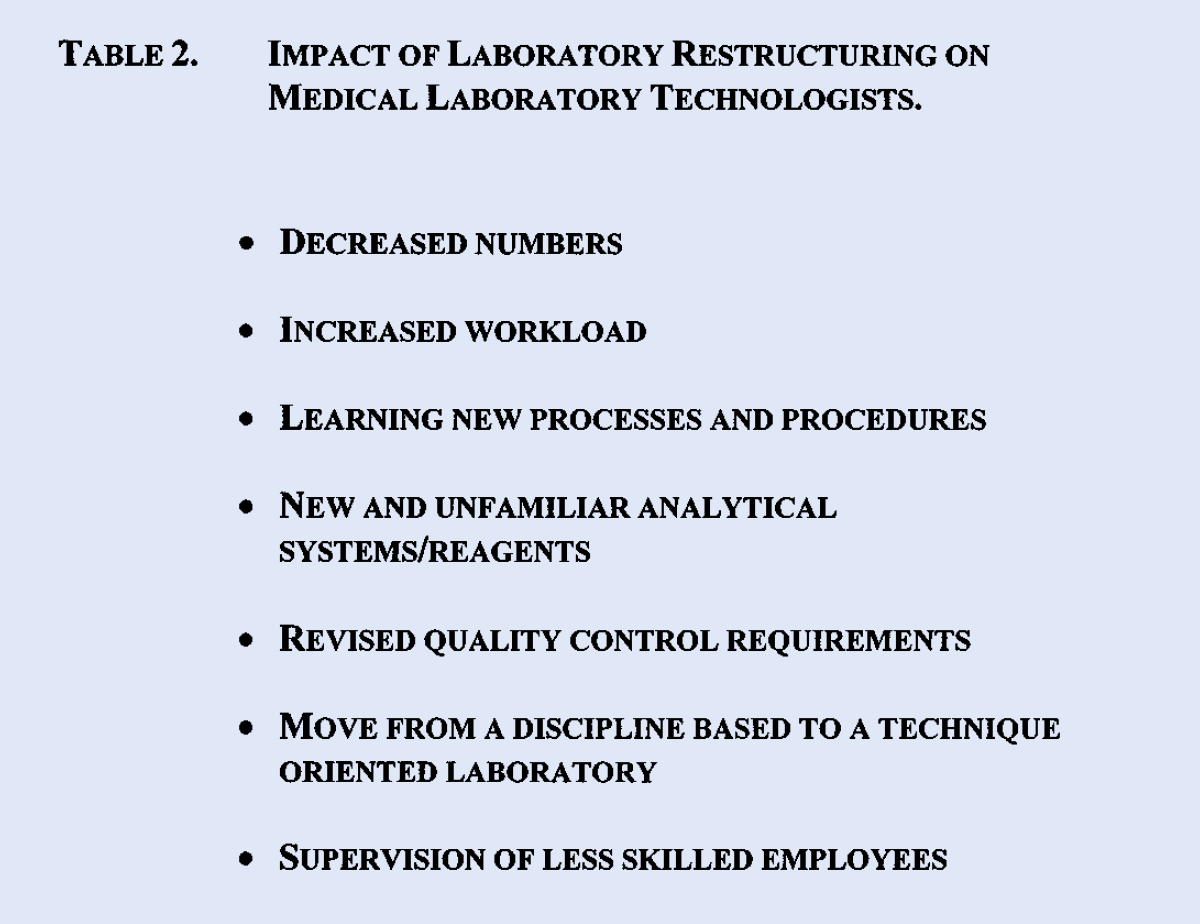
In Ontario, as in most other places where laboratory reorganization has taken place, the greatest impact has been felt by the medical laboratory technologists. The Ontario experience is similar to that in many parts of the world and is summarized in
IMPACT OF LABORATORY RESTRUCTURING ON MEDICAL LABORATORY TECHNOLOGISTS.
Restructuring has produced a reduction in the number of Laboratory Physicians and Scientists. This has made worse an existing shortfall in the numbers of these professionals. In 1988 the Royal College of Physicians and Surgeons of Canada recommended that there should be 52 Laboratory Physicians per million population. In Ontario, in 1996, there were only 39 per million. There is also a lack of recruitment into Laboratory Medicine training programs in Ontario. In 1997, there were 79 residents in these programs while there is an identified need for 115 new placements within 5 years and another 60 in the following 5 years. It is ironic that laboratory medicine has been further undermined by government restriction on funded postgraduate education positions. The number of placements for Laboratory Physicians over the next 10 years also reflects the fact that this is an aging group of physicians and there will be a large number of retirements in the next 5 to 10 years.
The situation is not significantly better for Laboratory Scientists. Their role in laboratory medicine has been inadequately appreciated and they have been relatively easy targets for cost reduction by elimination of their positions. The membership of the Canadian Society of Clinical Chemists has dropped by approximately 100 over a 3 year period. The population of Ontario is increasing as is the burden of illness, yet there are only 43 Clinical Chemists in the Province. Nine of them are over 55 years old and 3 are more than 60 years old. It is anticipated that even if none choose to take an early retirement before the age of 65 years, 20% of the Clinical Chemists will retire in the next 10 years. Faced with these numbers recruitment is a major problem, yet in 1997 only 5 trainees were enrolled in the 3 year Clinical Chemistry post-doctoral training programs in Ontario.
THE HAMILTON REGIONAL LABORATORY MEDICINE PROGRAM, A MADE-IN-HAMILTON SOLUTION
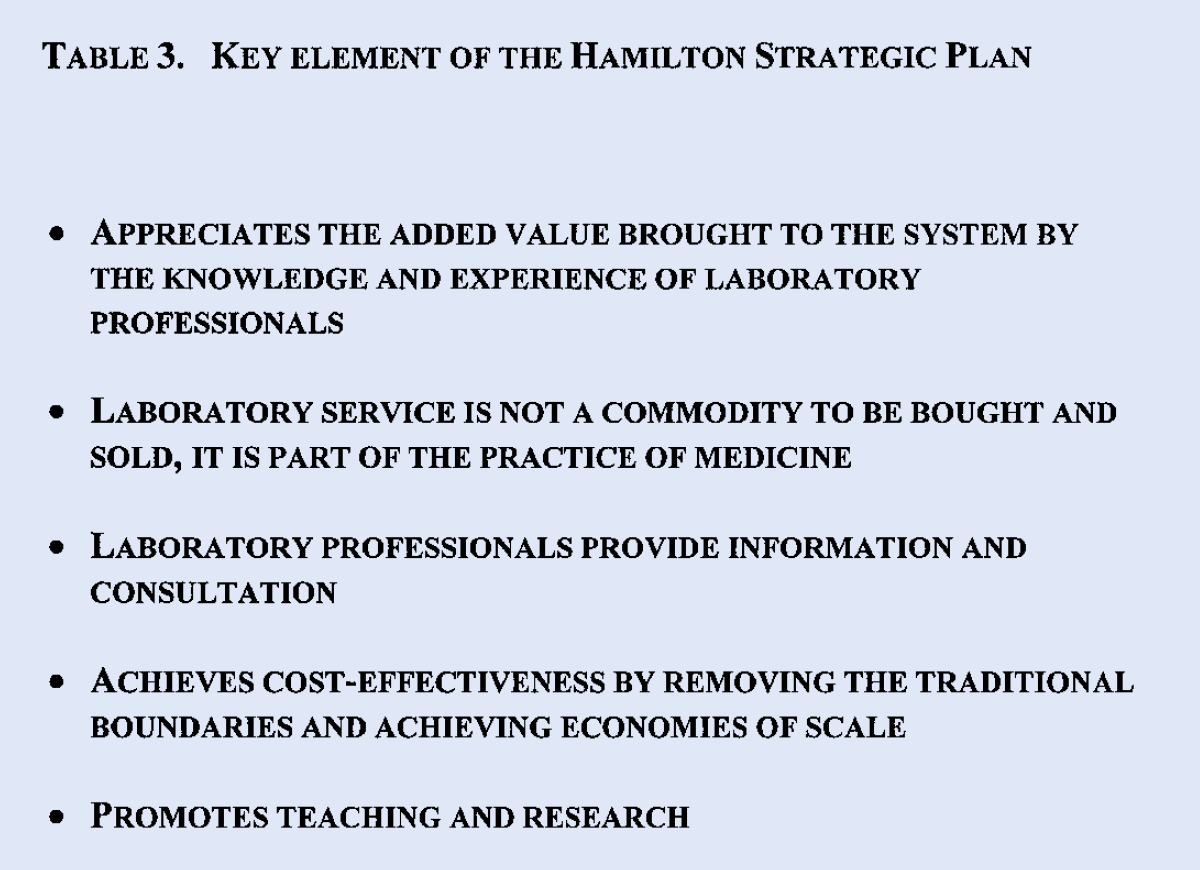
Recognising the need to be proactive rather than reactive(8), combined with a long history of cooperation and trust, brought together a multidisciplinary team of laboratory physicians, scientists, management, University and senior hospital administration. The key underpinnings of the locally developed strategic plan are in
KEY ELEMENT OF THE HAMILTON STRATEGIC PLAN
OUTLINE OF THE STRATEGIC PLAN

The agreed structure and relationships of the 4 hospitals within the Program are set out in
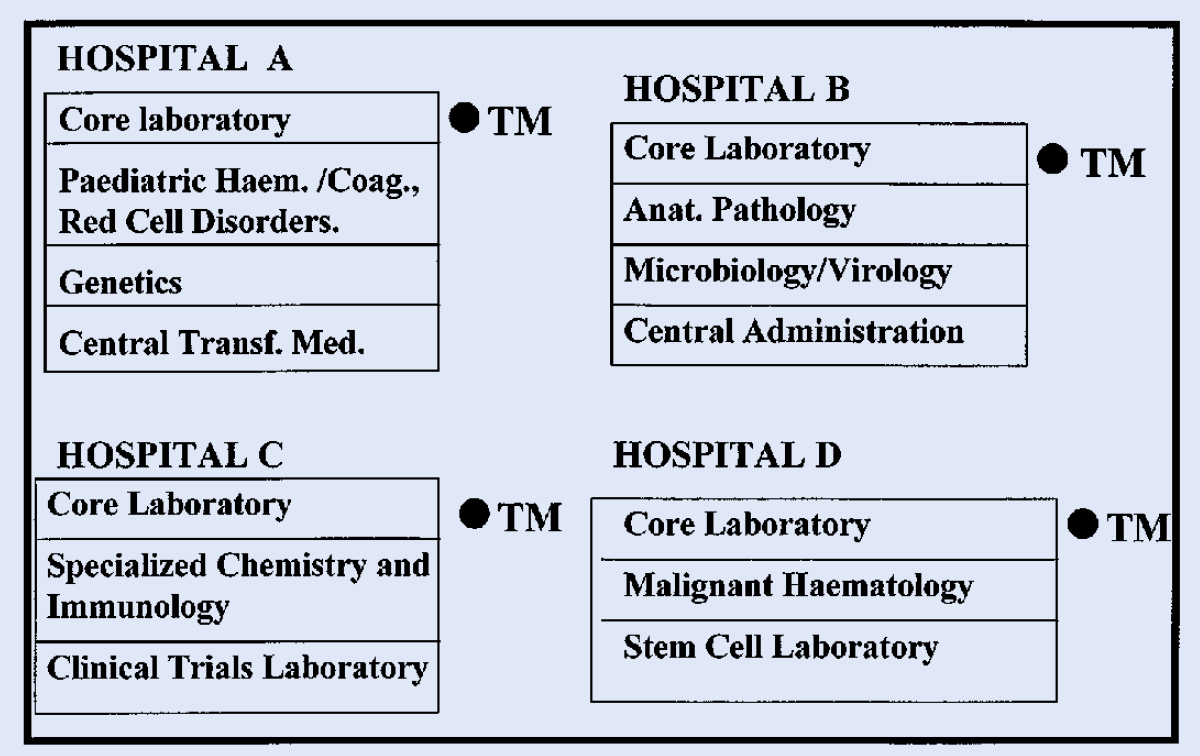
HRLMP AND DEPT. OF PATHOLOGY AND MOLECULAR MEDICINE
STATUS OF ‘WORK-IN-PROGRESS’
This plan requires major changes in a relatively short time. It is inevitable that some elements of the change will be accomplished more rapidly than others. From the beginning it was agreed that a single management structure, a comprehensive human resources solution that allowed for staff mobility, and a single Laboratory Information System (LIS) were 3 key enablers in the plan.
A summary of the current status of the reorganization activities is presented in point form in
A SUMMARY OF THE CURRENT STATUS OF THE SYSTEM RE-ORGANIZATION.

Although the construction of laboratory space is being kept to a minimum some is inevitable to accommodate centralized services which were previously provided at 3 or 4 sites. Some other changes are being driven by decisions concerning the locations of clinical programs. These follow the recommendations to Hamilton from the Ontario Hospitals Restructuring Commission which was established by the Ontario Government to direct the downsizing and reconfiguration of hospital services.
PROBLEMS IN IMPLEMENTATION
A reorganization of such magnitude is not without its problems. Not the least of these being the stress of coping with many changes in a short time. The staff have faced increased workload along with the anxiety and stress of coping with the introduction of a single laboratory information system, multitasking and the new analytical systems and reagents. One of the most important effects has been pressure from increased managerial responsibilities devolving to fewer managers. There is a real danger of burnout and we must be constantly sensitive to this potential problem.
As suggested earlier in the Ontario LPTP newsletter, we have recognized issues of maintaining good quality control and a system has been put in place to monitor this and to take appropriate action when this is identified.
While the introduction of the single LIS is exciting with enormous potential for improving clinical interaction, it does represent a large investment of people, energy and enthusiasm while at the same time having to work with and maintain 3 legacy systems. An enthusiastic team is making good progress with this. However, several of those individuals are the holders of much of the knowledge of the legacy systems and it is a management challenge to ensure that they are not becoming too distracted from the new project.
The presence of more than one union representing the laboratory staff limits the flexibility of moving technologists and secretaries from one site to another. A solution to this problem has been slow in development, partly because aspects of hospital and laboratory reorganization are new territory for government, hospital administration and the unions. There has also been a strong desire to respect the roles and responsibilities of all the parties involved and to work towards agreement rather than confrontation.
Even when two hospital corporations willingly cooperate, they have different traditions and values. Handling these is a challenge for HRLMP which reports to both yet requires a common set of policies and operating procedures.
CONCLUSION
The reorganization of the Hamilton Regional Laboratory Medicine Program is an experiment in integration and collaboration that has not been attempted anywhere else in Canada. Different approaches have been taken in the academic centres in most of the major cities in Canada but none have planned it along the lines adopted in Hamilton, nor did any of the centres have the same record of collaboration upon which to build. The challenges and problems have been openly stated. It is also clear that much has been achieved. Teaching and research has not been weakened but we need to experience the benefits of the reorganization otherwise the pressures on staff time will begin to erode our academic endeavors. There is a need to devote more time to redesigning our role in teaching and training laboratory professionals for the challenges they will face in the 21st Century(9). We need time to allow the changes to be fully assimilated and the benefits realized. It will probably take another 2 to 3 years to see if we have been successful. Many good initiatives have been started but their real success can only be tested by time. It is encouraging to us that in spite of all the challenges, so far we have not weakened the academic base or reduced our academic activities in teaching and research.