
Abstract


INTRODUCTION
Laboratory medicine has undergone many changes over the last two decades in terms of automation, information systems, the use of dry chemistry and the advent of point-of-care testing, just to mention a few. There is a major shift in emphasis at the present time. There is a strong focus on cost containment as reimbursement for testing is ratcheted down. In addition, “clinical resource management” has become the phrase of the moment. Clinical resource management stresses the need to evaluate what testing, either laboratory or diagnostic imaging, is actually necessary in any particular disease state. Predetermined pathways are designed so that in a disease such as asthma, the length of stay in the hospital and the testing modalities are predetermined, although obviously exceptions can be made in unusual circumstances.
PLANNING
In deciding the best way to effect cost containment an approach needs to be taken using a multiskilled team. This team should be composed of persons at all levels in the laboratory, from the phlebotomist to director. It is also important to involve staff from all shifts. Figure 1 shows the process by which such planing for cost effectiveness should take place. Once the team is selected to create the vision and the plan, they must describe both the vision and plan in clear terms. They must communicate the plan to all the laboratory staff and then, with the approval of the laboratory director, the plan should be implemented and the outcome assessed on an on-going basis.

The rules for planning a way to becoming cost-effective are numerous, but probably the most important are to consider change, to be innovative and to reengineer. It is important to develop a strategic plan, which should constantly be evaluated. Empowerment of staff to assist in the implementation of the plan is critical to its success and in managing the diversity of the people involved we must always think creatively and futuristically, and we must be aware of economic and other restraints. Planning, unfortunately, often fails because it lacks an implementation schedule and does not address three critical questions. These are:
What tasks need to be accomplished?
Who is responsible?
What resources are necessary?
As our team met to consider reengineering the laboratory, it considered several major factors. These included current and future trends in health care and testing, consolidation of services, human resource needs, technology, capital equipment, space and customer service.
CONSOLIDATION
It became clear fairly quickly that consolidating services would be the premier goal in bringing about cost containment. By consolidating our laboratory, the goal was to improve customer service, to develop more cross-training, a new plan for phlebotomy services, while increasing outreach business and maintaining our academic mission by increasing our number of publications per faculty member and increasing our dollars from research grants.
RESULTS
Figure 2 illustrates the structure of the laboratory as it was in 1995. There were nine separate technical sections supported by the laboratory information system, phlebotomy and operations (specimen receiving, handling and accessioning). Each area had its own director except that the director of the stem cell laboratory also handles transfusion medicine. There were ten directors; all had an MD or PhD degree. Each section had its own supervisor.
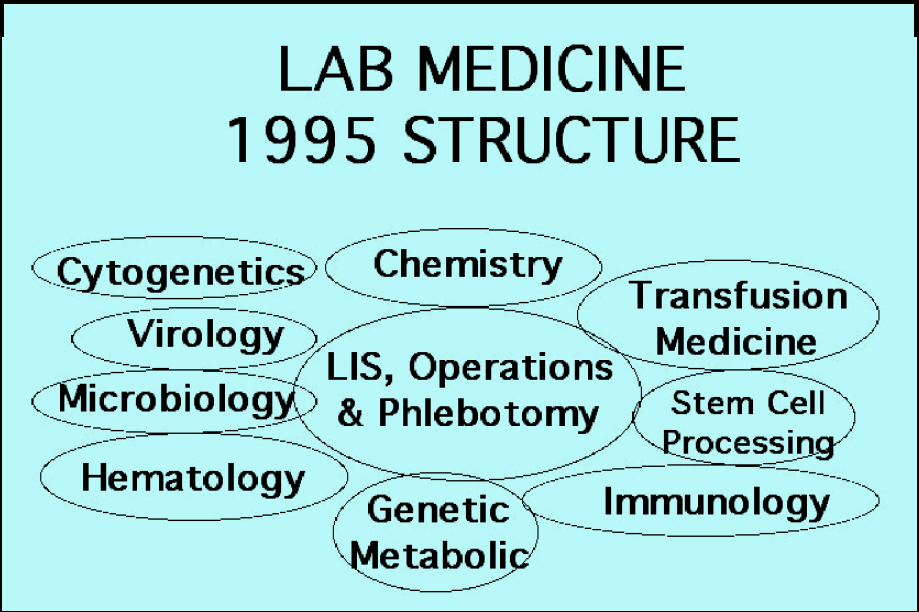
Figure 3 shows the current structure, which encompasses four major sections. Transfusion medicine has thus far been kept separate as it is quite complex because it is not only a transfusion service, but includes a blood donor service and a therapeutic pheresis service and stem cell laboratory, although the last named is to be transferred shortly to the hematology/oncology clinical department. Molecular diagnostics/biochemical genetics and microbiology/virology form two other sections. These areas were separated out because they are the major disciplines in which we planned to attract outreach business. All the rest of the testing which includes basic and specialized hematology/basic and specialized chemistry/immunology and microbiology incoming comprise the core laboratory.

This model for a consolidated laboratory achieved considerable savings by using space more efficiently, by decreasing the number of employees, both at the technical and director level (to 4.6), by changing the skill mix, and by moving considerable testing to point-of-care.
SPACE AND STAFFING
Space reconfiguration was essential to our success. We had to tear down many walls to achieve a large open core laboratory. Our central receiving area for specimens is close to the core laboratory and hematology, and clinical chemistry equipment is adjacent. We installed more computer terminals to effect better use of time so that personnel all had computers at hand. From 1995 to now we decreased our technical employees from one hundred to ninety, we changed the number of supervisors from nine to two and instituted coordinators who are several pay scales lower than supervisors. We also changed our skill mix dramatically from 12% MLTs/88%MTs to 40% MLTs/60%MTs. In the US, an MLT (Medical Laboratory Technician) has a two year Associates' degree or a high school diploma plus training in an accredited laboratory; an MT (Medical Technologist) has a four year Bachelor's degree plus training in an accredited laboratory. This obviously also helped in our cost savings.
A very aggressive move to point-of-care testing has also allowed us to save $200,000 per annum in technical salaries and to capture more billing. Currently, one third of our testing is done outside the central laboratory. It is under the total supervision of the Department of Laboratory Medicine from quality assurance to choice of equipment to competency assessment of the staff who mostly carry out the analyses. Our total saving in salaries by all these efforts was close to $2,000,000 over four years.
When staffing is reduced and finances are stressed it is easy to lose track of one of the most important elements of any business, and that is customer service. We decided to improve telephone answering, turn-around-time of results, the courtesy and helpfulness of our staff, the waiting time to have specimens drawn, and to make blood drawing available at our six regional outpatient centers most of which are more than 20 miles from our main hospital site in Washington, DC.
CUSTOMER SERVICE
Telephone standards
The standards we set for answering the telephone were to give the name of the department, one's own name and a pleasant greeting such as “may I help you?” In the last year, we have improved from 68% to 98% in giving the name of the department; from 20% to 80% in giving one's own name; and, from 5% to 57% in giving a greeting. We clearly answer the phone much more pleasantly, but there is still room for improvement.
TURN-AROUND-TIME
Our goal for turn-around-time was to have all basic hematology and chemistry results out within one hour of receipt in the laboratory on a consistent basis, but we have not achieved that. A brainstorming session a couple of months ago has caused us to make some changes to improve our turn-around-time dramatically. Some of the ideas implemented were a designated person to answer the telephone to avoid others from having to interrupt their work, designated phlebotomists to draw outpatient stats and to enter the information into the laboratory computer, emphasizing the team concept, moving computer terminals to be more accessible and improving our computer training especially of new employees.
COURTESY AND HELPFULNESS OF PHLEBOTOMISTS
We gave out questionnaires to all parents bringing children to our outpatient phlebotomy area to ask how well the phlebotomist treated them. In February 1999, 93% answered excellent, 6% good, 1% fair and 0% poor. We were pleased with this outcome.
WAITING TIMES
Using the same outpatient questionnaire, we asked whether parents had to wait less than 5 minutes, 5–10 minutes, 10–15 minutes or more than 15 minutes to have their child's blood drawn. By February 1999, 46% waited less than 5 minutes, 29% 5–10 minutes, 17% 10–15 minutes and 8% over 15 minutes. Since our standard was that no patient should wait more than 15 minutes, we still have some room for improvement.
CROSS-TRAINING
In beginning a program of training technologists from one discipline to another it is important to choose, first, persons who are team players, who have a positive attitude, who are open to change, who enjoy challenges and are generally good with instruments. This approach will lead to initial success of the program. Examples of areas in which to cross-train are chemistry/hematology, microbiology/virology, hematology/immunology and chemistry/microbiology incoming. Phlebotomists in the regional outpatient centers have been trained to also do simple point-of-care testing, EKGs, blood pressure and patient weights.
OUTREACH BUSINESS
In order to become more cost-effective it is also important to improve out-reach business and also look for opportunities to increase it. Some of the areas in which we have been successful include doing all the testing for other hospitals, doing virology and metabolic/genetic testing for other institutions, doing testing such as lead for community physicians, irradiating blood and doing stem cell preparation for other hospitals, and managing the cytogenetics laboratory at a local women's hospital.
ACADEMICS
In the current rather stressful environment in laboratory medicine it is important not to lose sight of the academic mission. We set a goal of publishing at least two peer-reviewed papers per faculty member per year. We exceeded this in 1998 and published 2.9 papers per faculty member. We also increased our grant portfolio.
SUCCESS OR NOT?
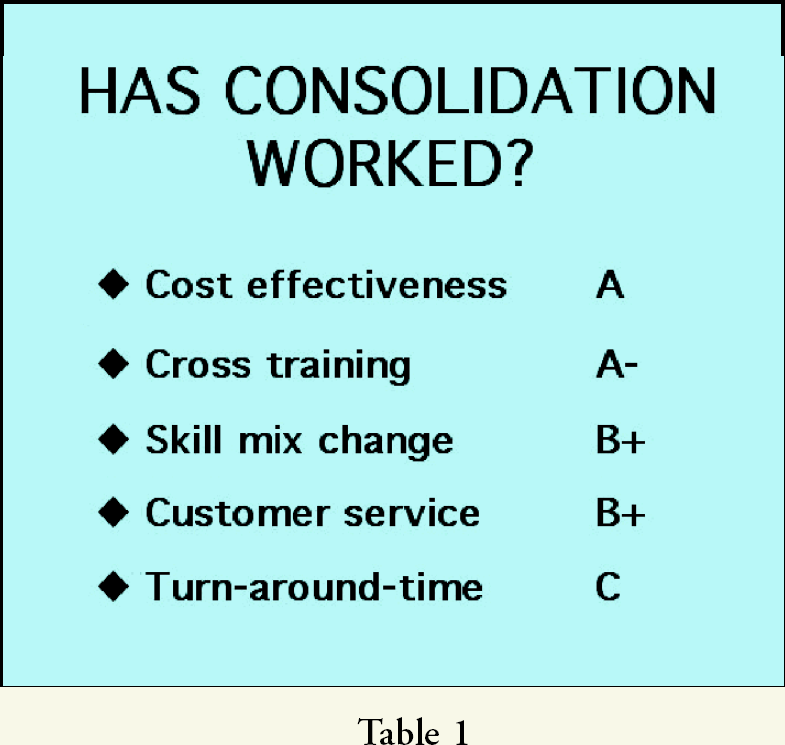
We graded ourselves on how well we achieved our goals in the consolidation of the laboratory, and the results are shown in Table 1.
HAS CONSOLIDATION WORKED?
LOOKING AHEAD
In order to continue our success and improve our cost-effectiveness we need to look for appropriate technology, assess our human resource needs and continue to increase our outreach business. We need to choose consolidated platforms to combine hematology/chemistry and immunochemistry testing. We need to be aware of new technology in point-of-care testing. We also should have good connectivity from all testing sites and should consider the use of telemedicine. In order to improve our outreach business, we must develop a larger armamentarium of tests in genetic and molecular diagnostics and consider programs of preventive testing. In terms of human resources, we need to continue to be aggressive in changing our skill mix and maintaining cross training, reward flexibility, continue to work with fewer staff and consider working from home.
COMMUNICATIONS
The key to success in any changing environment is to communicate well and often. It is important to hold regular meetings, to hold brainstorming sessions and use the e-mail. It is vital to be honest… to tell employees what works today, may change tomorrow.
In conclusion, two very well known and respected world leaders said it perfectly: “To improve is to change. To be perfect is to have changed a lot” Sir Winston Churchill.
“Change is the law of life, and those who look only to the past or present are certain to miss the future” John F. Kennedy.
My thanks go to Maria M. Chan, PhD, who led the team that developed the plan for a consolidated laboratory. Without her help none of our successes would have been possible.