
Abstract
This paper reports five new cases of intrathoracic tracheal rupture in cats, and summarizes these cases in conjunction with 11 cases from the literature. Most cats had no obvious respiratory signs at the time of injury, and in half of them the tracheal rupture was the only injury. The interval from trauma to onset of dyspnoea ranged from 1 to 28 days (median 12.5 days). Radiographic findings include loss of continuity of the trachea, often with a gas-filled diverticulum present between separated tracheal rings. With careful attention to surgical technique and anaesthetic management the prognosis for these cats is excellent. All eight of the cats reported in the last 14 years having surgical correction survived and returned to normal. The surgical anatomy, approach and tracheal anastomosis technique is described and recommendations for anaesthetic management are made.
Intrathoracic tracheal rupture in cats is a condition that has been reported sporadically in the literature, with only 11 cases reported since 1972. In many of the earlier case reports the cats either died or were euthanatized, suggesting a poor prognosis (Ryan & Smith 1972, Kennedy 1976, Feeney 1979, Brouwer et al 1984). However, in the two most recent clinical reports of four cats with this condition, all had a successful outcome with surgery (White & Milner 1995, Griffiths et al 1998).
Tracheal rupture occurs secondary to blunt trauma that typically involves hyperextension of the head or neck. As the carina is relatively fixed compared with the tracheal wall, hyperextension causes rupture of the trachea, generally just cranial to the carina. Due to the persistence of peritracheal tissue (either tracheal adventitia or mediastinum), continuity of the airway is retained. In many of the reported cases, the initial dyspnoea resolved with the cat re-presenting later (5 to 14 days) with severe dyspnoea.
This paper reviews the cases in the veterinary literature, and reports the clinical findings, management and outcome of a further five cases.
Case histories
Case 1
A 4-year-old male castrated domestic short-haired cat (DSH) was hit by a car and presented to the referring veterinarian. The cat was in shock, non-ambulatory, and had anisocoria. The left forelimb had lower motor neuron signs and a diagnosis of brachial plexus avulsion was made. The cat's condition gradually improved, although 2 weeks following trauma an increased respiratory rate and dyspnoea were noted. Thoracic radiographs were not done at this time. Four weeks after trauma the left forelimb was amputated. The cat's breathing did not improve and it was referred for evaluation of dyspnoea 8 weeks after trauma. On presentation at that time the cat displayed marked dyspnoea and stridor. Harsh inspiratory sounds were auscultated over the thorax, and increased sounds were present over the upper airway and larynx. Thoracic radiographs done on presentation are shown in Fig 1.

Lateral (a) and ventrodorsal (b) radiographs of case 1. On the lateral view, hyperinflated lung fields and interruption of the intrathoracic trachea with an oblique soft tissue band, approximately 3 mm thick at the level of the fourth rib, are revealed.
The cat was premedicated with ketamine (5 mg/kg im) (Parnell Laboratories) and acepromazine (0.02 mg/kg im) (ACP. 2: Delta Laboratories), and anaesthesia was induced with thiopentone (10 mg/kg iv) (Pentothal, Boehringer Ingelheim Pty Ltd, Artarmon, NSW, Australia) and maintained using isoflurane (Forthane, Abbott Australasia) and oxygen. Upper airway endoscopy was performed. The larynx, pharynx, and cranial trachea were assessed as normal. In the caudal trachea two areas of constriction were evident as concentric rings of pale tissue. Between the narrowed areas tracheal rings were not visible, and the tracheal lumen was almost obliterated on inspiration, and approximately 50% of normal diameter on expiration.
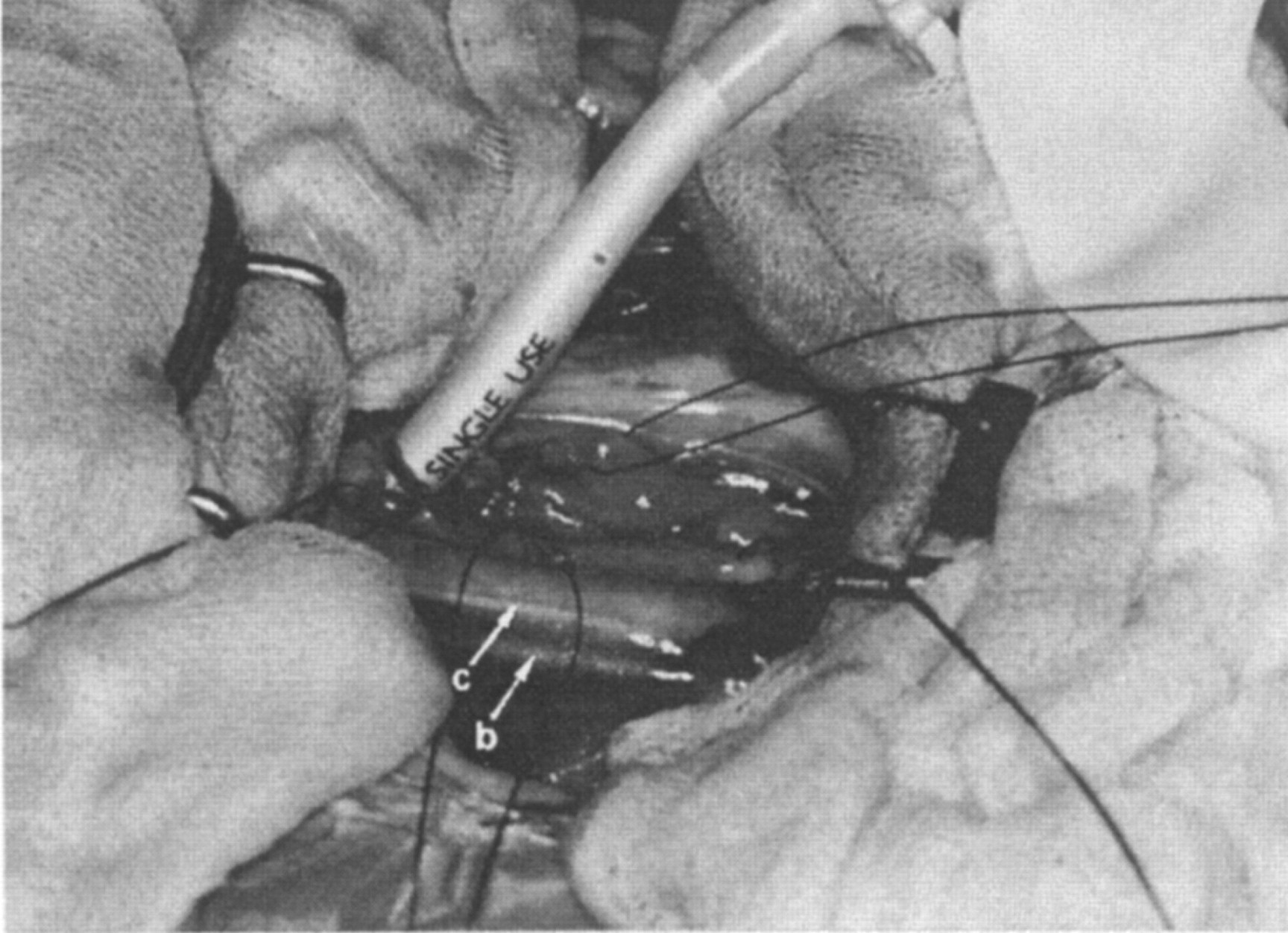
The trachea was approached via a right fourth intercostal thoracotomy. Normal tracheal rings were apparent cranially and caudally, with a ballooning pseudotrachea that had a stricture at each end (Fig 2). The pseudotrachea was incised and the caudal trachea intubated with a sterile endotracheal tube inserted through the thoracotomy incision (Fig 3). The pseudotrachea was dissected free and one tracheal ring cranially and caudally was removed. The endotracheal tube was re-inserted orally past the surgery site, at which time it was noted that the left arytenoid cartilage lacked abduction. The trachea was anastomosed with simple interrupted sutures of 1.5 metric polypropylene (Prolene; Johnson & Johnson Medical) penetrating adjacent cartilage rings. The thorax was filled with warm saline to ensure that there was no air leakage, a thoracostomy tube was placed, and the chest closed routinely.

Intraoperative view, case 1. A right 4th intercostal thoracocomy has been performed, and the mediastinum has been incised. The cats head is to the right of the photograph. The azygos vein (a) is present at the caudal extent of the surgical field, the cranial vena cava (b) and vagus nerve (c) are ventral to the trachea. The ballooning pseudotrachea (d) and distal trachea (e) are visible. Stay sutures are present in mediastinal tissue.
The cat recovered uneventfully, with no stridor ausculted and no increase in thoracic sounds. Radiographs 6 months after surgery showed no evidence of narrowing at the site of tracheal anastomosis (Fig 4). The cat remains normal 40 months after surgery.
Intraoperative view, case 1. The stenotic area has been excised and the distal trachea intubated with a sterile endotracheal tube. The cats head is to the right of the photograph, and surgical landmarks are as in Fig 2. An additional stay suture has been placed in the dorsal wall of the pseudotrachea.

Lateral radiograph of case 1 taken 6 months after tracheal resection and anastomosis.
Case 2
A 10-month-old male castrated DSH was presented soon after being hit by a car. The cat was in mild shock, weakly ambulatory and moderately dyspnoeic, and was treated with IV Hartmann's solution. Thoracic radiographs were considered unremarkable and the dyspnoea resolved over 24 h with cage rest. After a further 24 h observation the cat was discharged with instructions for moderate confinement.
Five days later the cat was re-presented for an acute onset of severe dyspnoea. Mucous membranes were cyanotic and the cat was open-mouth breathing with rapid, vigorous chest movements. Thoracic radiographs revealed hyperinflated lung fields and an apparent narrowing of the trachea 2 cm cranial to the carina. Review of the previous radiographs also showed a slight narrowing of the trachea at the same point.
Anaesthesia was induced using halothane (Halothane B.P.; Veterinary Companies of Australia) delivered in 100% oxygen via a facemask. The cat was intubated and the thoracic trachea approached via a right fourth lateral thoracotomy. A pseudotrachea of thickened mediastinum was observed spanning a 2 cm gap in the trachea. This area was opened and a second sterile endotracheal tube was passed into the distal trachea via the thoracotomy incision to continue ventilation. The area was dissected and the ends of the trachea were identified. The cat was re-intubated orally and the trachea was sutured with simple interrupted sutures of two metric polygylcolic acid (Dexon; Sherwood-Davis & Geck) encircling adjacent cartilage rings. The thickened mediastinum was lightly opposed over the anastomosis to help provide an airtight seal. The endotracheal tube cuff was deflated and the tube moved proximal to the anastomosis to continue ventilation. A thoracostomy tube was placed and closure was routine.
The cat recovered well from surgery and was not dyspnoeic. Thoracic radiographs 2 weeks post-operatively revealed only slight narrowing of the trachea at the anastomotic site. The cat is still without complications 7 years later.
Case 3
An 8-month-old intact female DSH presented to the referring veterinarian after being hit by a car. The cat was treated for shock and pulmonary contusions and intrathoracic tracheal rupture was diagnosed on thoracic radiographs. The cat was discharged from the hospital. Four days later the cat represented with an acute onset of dyspnoea and coughing, and was referred for further treatment. On presentation the cat showed marked dyspnoea and stridor, which was aggravated when the cat was examined or restrained. Radiography revealed a tracheal rupture approximately 2 cm cranial to the carina and a gas filled diverticulum between the second and fifth rib (as in case 5). Anaesthesia was induced with ketamine (5 mg iv) and propofol (4 mg/kg iv) (Dexon; Sherwood-Davis & Geck). The cranial trachea was intubated and anaesthesia maintained with isoflurane (Forthane, Abbott Australasia Pty Ltd) in 100% oxygen. A right fourth intercostal thoracotomy was performed. The ballooning pseudotrachea was incised, the ends of the trachea were cleaned of fibrous tissue, and the endotracheal tube was advanced past the rupture and into the distal trachea. The tracheal ends were anastomosed with simple interrupted sutures of 1.5 metric polybutester (Novofil; Sherwood-Davis & Geck) penetrating adjacent tracheal rings. A second row of tension sutures was placed using the same suture material. The thoracic cavity was filled with warm saline to ensure there was no air leakage at the anastomotic site. The mediastinum was left open, a thoracostomy tube was placed and closure was routine.
Respiratory stridor was present after surgery and a thoracic radiograph 2 days after surgery revealed peritracheal swelling. The cat improved within the next 2 weeks and radiographs 3 weeks after surgery showed only a slight narrowing of the trachea at the anastomosis without any increase in thoracic sounds or signs of dyspnoea. The cat remains normal 16 months after surgery.
Case 4
A 4-year-old female DSH presented immediately after being found collapsed in the owners yard. There was blood on the front legs and around the head, and the cats claws were frayed. Moderate dyspnoea and pale mucous membranes were evident on physical examination, and the cat was lame in the right hindleg from an unspecified soft tissue injury. A provisional diagnosis of pneumothorax was made. Oxygen was administered by face mask and later nasal insufflation, and the cat was treated for shock. Thoracic radiographs revealed a tracheal rupture 1.5 cm cranial to the tracheal bifurcation
Anaesthesia was induced with thiopentone (10 mg/kg iv) the next day and the cranial trachea was intubated. Anaesthesia was maintained with halothane in 100% oxygen. A right fourth lateral thoracotomy was performed and the endotracheal tube was advanced by the surgeon past two tears identified in the trachea, two rings apart, one ventrally and one dorsally. The tears were closed with simple interrupted sutures of 1.5 metric polypropylene. As the tears were very close to the carina the cuff of the endotracheal tube was positioned at the site of repair, and was accidentally perforated, which made IPPV difficult. Immediate post-operative radiographs showed narrowing at the anastomotic site (approximately 75% of normal), but the cat made an uneventful recovery and was discharged 1 week following surgery. She has remained normal for the last 20 months.
Case 5
A 9-month-old DSH was presented with dyspnoea. Thoracic radiographs are shown in Fig 5. The cat was treated with supportive care and cage rest, and the dyspnoea resolved within a few days. The cat was clinically normal at that time, and the owners declined surgical correction and took the cat home. At last follow-up 6 months after first presentation, the cat was clinically normal.

Lateral (a) and ventrodorsal (b) radiographs of case 5 revealed interruption of the trachea with a gas filled diverticulum present at the level of the second to fifth rib.
Results
The signalment, clinical and radiographic findings, and outcome of 16 cases, five from this report and another 11 cases in the literature, are detailed in Table 1. The mean age of all affected cats was 2.7±2.4 years (mean±standard deviation, range 4 months to 10 years, median 24 months). All but one cat had a history of recent trauma (eight vehicular trauma, one dog attack, one fall, and five unknown traumas). The time interval from trauma to onset of dyspnoea was from 1 to 28 days (mean±standard deviation, 10.7±7.9 days, median 12.5 days). Concurrent injuries were reported in eight of the 16 cats. Four cats had injuries to the thoracic limbs (two lacerations, one brachial plexus avulsion, and one cat with unspecified soft tissue injuries and a dislocated mandible), one cat had a soft tissue injury to a hindlimb, one cat had pulmonary contusions, one cat had liver trauma, and one cat had fractures of the right first to sixth ribs.
Summary of 16 cases
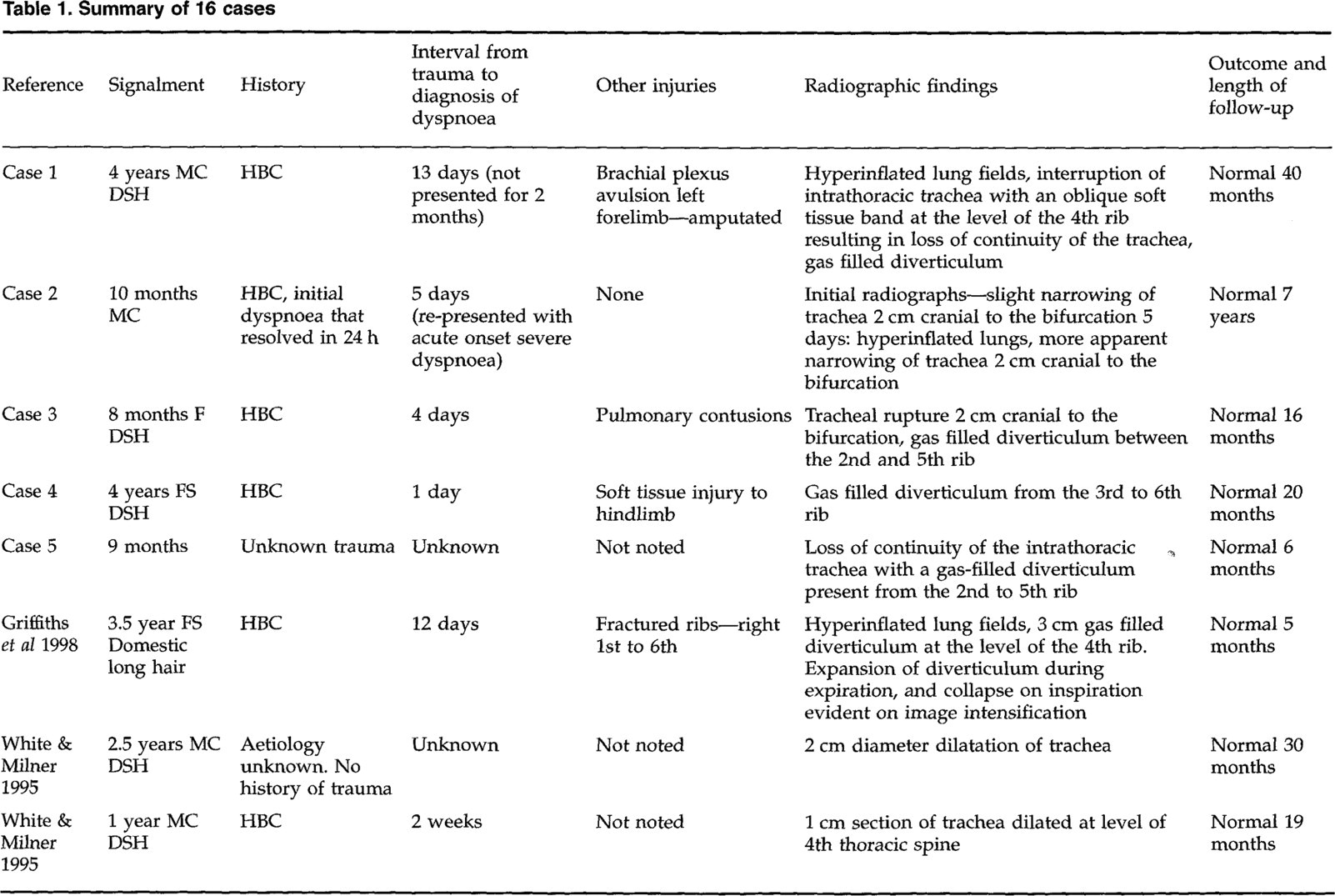

HBC—hit by car, MC—male castrated, FS—female spayed, F—intact female, M—intact male.
The most common radiographic appearance of the trachea, seen in eight cats, was loss of continuity, often with a gas filled diverticulum present between separated tracheal rings. Apparent narrowing or stenosis of the trachea was another common radiographic finding, being observed in five cats. Dilatation of the trachea was seen in two cats. One cat was not radiographed.
Of the 11 cats that had surgery, nine had an excellent outcome, being clinically normal at follow-up ranging from 5 months to 7 years. One cat was euthanatized at surgery due to anaesthetic difficulties, and one cat died intra-operatively. Of the remaining five cats, one did not have surgery and was alive at 6 months, one was found dead, and three were euthanatized at the time of diagnosis.
Discussion
Intrathoracic tracheal rupture is an uncommon injury in the cat but one which veterinarians should be aware of. It is primarily seen in young adult cats as they are more likely to be victims of vehicular trauma. Rupture typically occurs near the carina or at the thoracic inlet and may be due to violent hyperextension of the neck. The carina and lungs are relatively fixed in relation to the tracheal wall and as the trachea is stretched against this point it may rupture just cranial to the carina (Nelson 1993).
The injury is often not fatal and the tracheal disruption may not be evident on initial radiographic examination, or the changes may be subtle and overlooked as in case 2. Careful evaluation of initial radiographs is important. Once the cats have severe respiratory signs, radiographic changes are more obvious and include discontinuity or apparent narrowing of the trachea. The tracheal injury is thought to act as a partial one-way valve, allowing air into the lungs but partially preventing its escape. Radiographically this corresponds to an appearance of hyperinflated lung fields.
Of the 16 cats reviewed in this paper, 13 cats had no obvious respiratory signs immediately following trauma (most of these were examined by a veterinarian) and in eight of them the tracheal rupture was the only injury sustained as the result of the trauma. Most cats were re-presented at a later time (mean 10.7 days) because of a sudden onset of severe dyspnoea. It appears that when the trachea is ruptured, a thin membrane of adventitia may remain intact connecting the two separate ends and maintaining a patent airway. It is reported that recently ruptured tracheal segments have not dilated and formed a pseudoairway (White & Milner 1995). Development of the pseudo-airway is a sign of chronicity, and is possibly associated with changing airway pressures produced by progressive stenosis of the cranial and caudal ruptured tracheal ends. When this occurs, or when the tracheal ends become displaced, dyspnoea returns or worsens (Nelson 1993). This delay in the onset of clinical signs highlights the need for routine thoracic radiography following significant trauma, and the importance of monitoring all cats following thoracic trauma, including those with initial dyspnoea that then resolves.
Surgical correction should be performed as soon as possible, as chronic stenotic lesions in the trachea can cause secondary degenerative changes in the distal trachea, bronchial tree and lungs (Nelson 1993). As evidenced in case 1, chronicity can also make identification of important structures more difficult. In these cases between 0 and 8 tracheal rings were excised (there are about 40 tracheal rings in cats; Nelson 1993). In the dog it is reported that 25 to 50% of the trachea can be resected without dehiscence and stenosis (Nelson 1993), but similar figures are unavailable for the cat. The best method for tracheal anastomosis in cats is a simple interrupted suture pattern that penetrates the cartilage rings adjacent to the incision. Tracheal ring encircling sutures can be used, but there is more of a tendency for the segments to override (Nelson 1993). None of the cats had any clinical signs of stenosis after tracheal resection and anastomosis, although mild stenosis at the site could not be ruled out without endoscopic examination, and was in fact seen on postoperative radiographs in case 4. Even though one case (case 5) became clinically normal with only cage rest, conservative management of tracheal rupture is generally not recommended because of the potential for respiratory signs to worsen over time.
Anaesthetic management of these cases is critical. Most of these cats had dyspnoea at rest, suggesting that the tracheal lumen was only 10 to 15% of normal diameter (Nelson 1993). These cats do not have a large respiratory reserve and any stress can exacerbate their respiratory distress and result in death. Pre-operative management includes premedication, which will reduce increased respiratory effort associated with excitement, and pre-oxygenation (Quandt & Raffe 1993). Anaesthetic intubation should be rapid to achieve early control of the cat's breathing. Intravenous induction agents are preferred over mask induction. Even though one of the cats in this report (case 2) was mask induced with halothane, this method of induction is not recommended as it may be stressful for the cat and it will take longer to achieve intubation. The anaesthetic protocol that we recommend is premedication with a short acting opioid, e.g. fentanyl, oxymorphone or butorphanol, and diazapem, pre-oxygenation via a face mask if the cat will allow it, rapid induction with either propofol or thiopentone, and maintenance with isoflurane and 100% oxygen. Because ketamine can predispose to bronchoconstriction, it may not be the best choice for induction. Nitrous oxide should not be used since the oxygen level should be maximized during thoracotomy.
A range of measured endotracheal tubes should be available (both cuffed and uncuffed), with several of the smaller sizes being sufficiently long enough to pass the site of tracheal rupture if necessary in an emergency. It is recommended not to attempt to pass the endotracheal tube past the lesion at anaesthetic induction, but to allow the surgeon to pass the tube into the distal trachea under direct guidance. This will avoid accidental perforation of the pseudotrachea and subsequent pneumothorax or pneumomediastinum. A pulse oximeter is a useful part of the anaesthetic monitoring protocol, and is also useful in the post-operative period to ensure that there is no airway obstruction after extubation.
The technique used in three of the cats in this report and in White and Milner's series (intubation of the caudal trachea with a sterile endotracheal tube delivered through the thoracotomy incision following incision of the caudal end of the stenotic area, and oral reintubation when the entire stenotic area was resected) was simple and required only a sterile endotracheal tube as additional equipment. The anaesthetic tubing can be threaded through a sterile sleeve to prevent it from contaminating the surgical field. When the distal trachea is reintubated orally the cuff of the endotracheal tube should ideally go past the site of anastomosis to allow IPPV and to prevent leakage of anaesthetic gases. Use of high frequency jet ventilation has been reported in the anaesthetic management of one cat with tracheal stenosis (Whitfield et al 1989), with the reported advantages of providing optimal access to the circumference of the trachea, an unobstructed surgical field, decreased surgery time and lower peak airway pressures. This technique requires specialized equipment that is not available to most veterinary surgeons. Griffiths et al (1998) reported use of a 6 French urinary catheter passed orally down the endotracheal tube and into the distal tracheal segment. This was then used as a guide to allow an uncuffed endotracheal tube to be advanced into the distal segment, providing an unobstructed view of the surgical field.
Surgical anatomy is very important. A right lateral thoracotomy at the fourth intercostal space provides the best access. Structures in the area to be identified and avoided include: the azygos vein (caudal to the surgical field), the cranial vena cava (ventral to the trachea), the right vagus nerve (lateral to the trachea), and the left recurrent laryngeal nerve (left ventrolateral aspect of the trachea). The azygos vein can be ligated and transected if necessary. In the cat with the 2-month clinical duration (case 1) it was very difficult to identify the left recurrent laryngeal nerve (note that the right recurrent laryngeal nerve is cranial to the surgery site as it travels around the right subclavian artery from the right vagus nerve, and thus would not be encountered). The observation by the anaesthetists at the time of replacement of the oral endotracheal tube that the left arytenoid was not abducting is evidence that the recurrent laryngeal nerve was damaged. Damage may have been at the time of the initial trauma or possibly during surgical resection of the pseudotrachea. Initial endoscopy of the upper airway in this cat was reported to be normal, but the cat was at a deep level of anaesthesia to allow endoscopy, making assessment of laryngeal function difficult. Eight months later this cat was anaesthetized for removal of a small dermal mast cell tumour and the left laryngeal paralysis had not resolved. The cat showed no clinical signs of laryngeal hemiplegia and was able to exercise and play normally.
In conclusion, with timely diagnosis, careful anaesthetic technique, and a good knowledge of the surgical anatomy the prognosis for these cats is excellent. Complications seen in this case series include radiographic post-surgical narrowing of the tracheal diameter (three cats) and left laryngeal hemiplegia (one cat). Both of these complications were clinically insignificant. All nine of the cats reported in the last 14 years having surgical correction survived and returned to normal.