
Abstract
Twenty-four specific-pathogen-free-derived cats aged four to 11 months were challenged by ocular application of a field isolate of Chlamydia psittaci to evaluate the effect of topical and systemic therapy on the course of disease. The cats were monitored for 35 days post-challenge, with severity of clinical signs being measured using a scoring system, and ocular shedding of the organism monitored by culture of conjunctival swabs. All cats developed active C psittaci infection, and after 7 days the cats were randomly assigned to one of four treatment groups: Group P (placebo) was given twice-daily ophthalmic tear-replacement ointment; group F was given twice-daily topical 1% fusidic acid ophthalmic viscous drops; group C was given twice-daily topical 1% chlortetracycline ophthalmic ointment; and group D was given doxycycline at 10 mg/kg daily per os in addition to twice-daily topical 1% fusidic acid ophthalmic ointment. Within 24 h of commencement of therapy, group D had significantly lower median clinical scores than group P, and with the exception of day 16, this trend was maintained throughout the observation period. Median clinical scores of cats in group F were not appreciably different to those in group P, whereas the median scores of cats in group C generally fell between those of groups P and D. The median duration of C psittaci shedding was 10 and 15 days for groups D and C respectively, but four of the six cats in groups F and P were still shedding organisms at the end of the study (day 35). In this study, systemic therapy with doxycycline proved superior to topical therapy in the treatment of feline chlamydiosis.
In both the UK and elsewhere, Chlamydia psittaci has been established as a common feline pathogen, and an important cause of conjunctivitis in this species (Shewen et al 1978, Cello 1971, Studdert et al 1981, Wills et al 1988, Gunn-Moore et al 1995).
Although therapy with tetracyclines has been widely regarded as the treatment of choice for feline chlamydiosis, there has been disagreement on whether topical ophthalmic preparations, systemic antibiotics or combination of the two is preferable for therapy (Shewen et al 1978, Cello 1971, Pedersen 1988, Szymanski & Latimer 1989, Dorin et al 1993, O'Dair et al 1994, Wills & Gaskell 1994). This lack of consensus on optimal therapy is due, in part, to a lack of data available from controlled experimental trials evaluating therapeutic agents.
The purpose of this study was, therefore, to compare a licensed topical therapy (chlortetracycline ophthalmic ointment) with a licensed systemic therapy (doxycycline) and a placebo therapy (topical ophthalmic lubricating therapy) for the treatment of experimentally-induced feline chlamydiosis. In addition, as the authors were aware that topical fusidic acid has been used off-label in practice to treat feline chlamydiosis (unpublished observations), a fourth-treatment group was incorporated to evaluate the efficacy of this preparation. Furthermore, as we had previous experience of doxycycline as a sole therapy (Sturgess et al 1996) topical fusidic acid was also added to the doxycycline treated group.
Materials and methods
Experimental infection
Twenty-four healthy, specific-pathogen-free-derived, domestic shorthair cats were used which were all seronegative for C psittaci antibodies by indirect immunofluorescence (O'Dair et al 1994). There were 21 females (all entire) and three males (all neutered), their ages ranged from 4 to 11 months (median 9 months) at the start of the trial. The cats were housed in three rooms, each containing between six and 12 individuals.
On day 0, each cat was challenged with C psittaci by bilateral ocular application of 25 μl of a suspension containing 4×105 inclusion forming units per ml. The isolate used for the inoculation (C1418) was obtained through the Feline Diagnostic Service at the University of Bristol, from a naturally-occurring clinical case of feline chlamydiosis and was prepared for inoculation as previously described (Wills et al 1987, O'Dair et al 1994).
Treatment and monitoring
From 3 days prior to challenge (day −3) until day 35, the cats were examined at least three times weekly (on days −3, 0, 2, 4, 7, 8, 9, 10, 11, 14, 16, 18, 21, 23, 25, 28, 30, 32 and 35). On each occasion, a conjunctival swab was collected from the right eye for chlamydia isolation, while the left eye was evaluated for clinical disease.
Conjunctival swabs were placed immediately in chlamydia transport medium (Spencer & Johnson 1983) and stored at −20°C until cultured using previously described methods (O'Dair et al 1994, Wills et al 1986).
The severity of clinical disease was monitored using a modification of a previously described scoring system (O'Dair et al 1994), that incorporated evaluation of 15 specific ocular and non-ocular signs. The ocular signs scored were: conjunctival congestion, chemosis and follicular change; third eyelid protrusion, congestion, and follicular change; serous and mucopurulent ocular discharge; blepharospasm and eyelid swelling. The non-ocular signs scored were: respiratory signs (e.g. nasal discharge), submandibular lymphadenomegaly, other peripheral lymphadenomegaly, depression/lethargy, and inappetence. For each of the 15 signs, the cats were given a subjective score of between 0 (normal) and 3 (very severe) with scoring intervals of 0.5. Total clinical scores for individual cats at each time point were derived from the sum of scores for the individual signs. The scorer was blinded to the treatment received by the individual cats.
On day 7, the cats were randomly assigned to one of four treatment groups (six cats in each): group P were given topical placebo (tear replacement) therapy (Lacri-Lube; Allergan) 200–300 μl applied to both eyes twice daily; group C were given topical 1% chlortetracycline hydrochloride (Aureomycin Ophthalmic Ointment; Willows Francis Veterinary) 200–300 μl applied to both eyes twice daily; group F were given topical 1% fusidic acid (Fucithalmic Vet; Leo Animal Health) 200–300 μl applied to both eyes twice daily; and group D were given a combination of systemic doxycycline (Ronaxan; Merial) at 10 mg/kg once daily with topical fusidic acid as described. Treatment was maintained for the remainder of the trial (4 weeks). As separate rooms were not available for all four treatment groups, the cats were randomly assigned between the three rooms used.
Statistical analysis
Differences in median clinical scores between treatment groups at the various time points, and differences in median duration of C psittaci shedding between treatment groups were assessed with a Kruskall-Wallis test, using Dunn's post-test analysis to identify specific treatment groups that varied significantly. A P value of <0.05 was considered significant.
Results
Prior to challenge with C psittaci, no chlamydia were isolated from ocular swabs, and clinical scores were zero or close to zero in all cats (Figs 1 and 2). By day 2 post-challenge, C psittaci was isolated from two of the cats, and by day 7, swabs from all cats were positive (Fig 2).
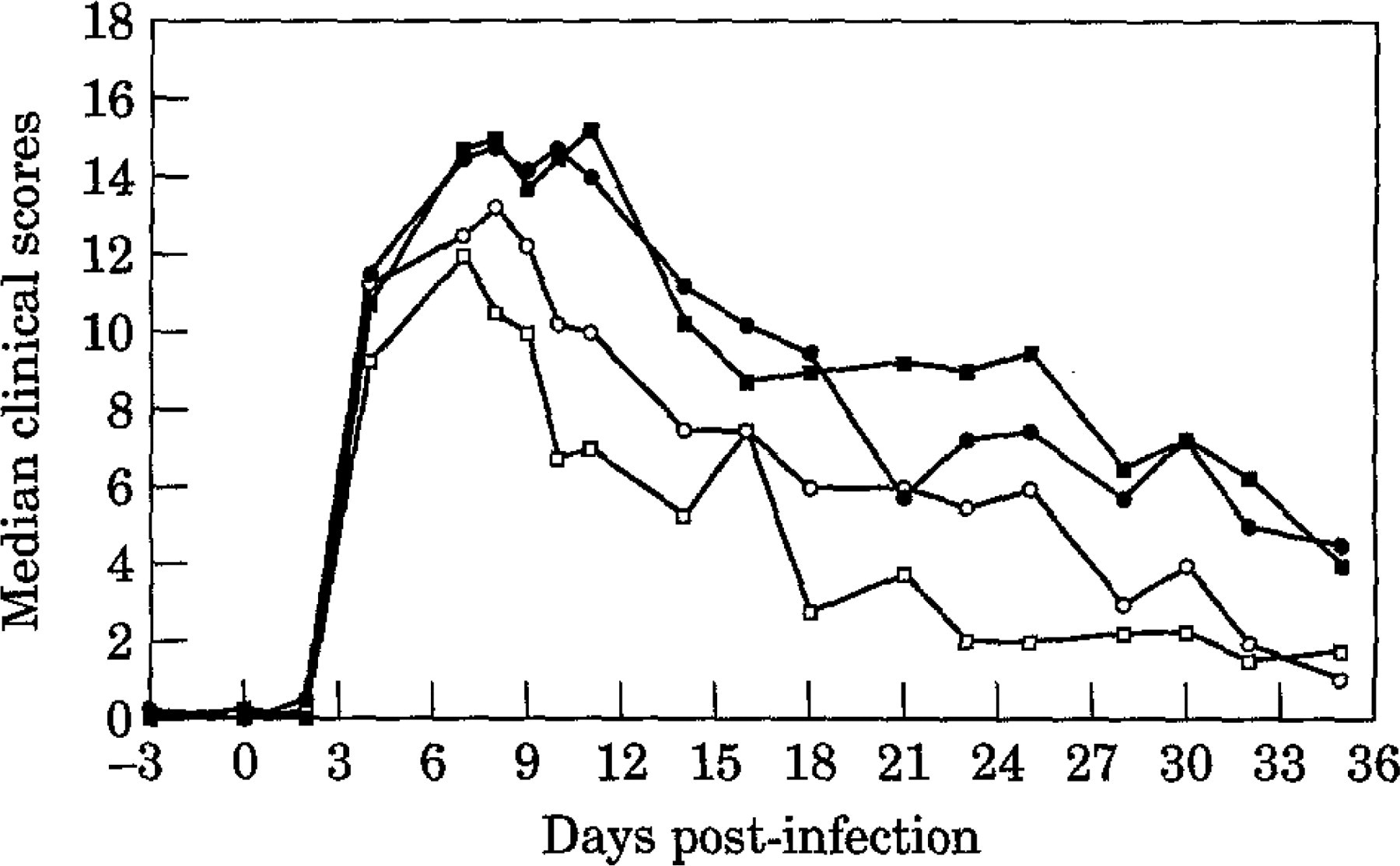
Median clinical scores in the four treatment groups (treatment started on day 7). Key: ▪, Group P; □, Group D;, Group C; ○, Group F.

Chlamydia isolation from ocular swabs in the four treatment groups (treatment started on day 7).
Randomization of the cats into the four treatment groups at day 7 yielded no significant difference in the median clinical scores between the groups. However, within 24 h of commencing treatment, significant differences were evident, and with the exception of day 16, these remained significant (P≤0.011) until the end of the study (day 35, Fig 1). Employing Dunn's post-test analysis revealed that, apart from day 16, throughout days 8 to 35 (inclusive) group D had significantly (P<0.05) lower median clinical scores than group P, and that in addition, on days 9, 11, 14, 18, 23, 30 and 32 group D had significantly lower median scores than group F. There were no significant differences at any time point between groups F and P or between groups C and D although there was a trend (Fig 1) for group C to have higher median clinical scores than group D. This is reflected in the fact that apart from day 32, there were no significant differences between groups P and C.
By day 11 (after 4 days of treatment), all cats in group D were negative for C psittaci by culture of ocular swabs (Fig 2), whereas 17 of the other 18 cats were still infected (positive swabs). Table 1 shows the duration of C psittaci shedding in individual cats. Eight cats (all in groups P and F) were still shedding at the end of the trial (day 35). Statistical composition between the four groups demonstrated a significant difference (P = 0.0003) in the median duration of C psittaci shedding, with group D having a significantly shorter median shedding period than either groups P or F (P < 0.05). Furthermore, although one cat from group D was positive on culture at day 25, this cat had previously been consistently culture negative from day 10 onwards. As the four treatment groups were not kept physically separate, the isolated positive culture on day 25 from this cat may therefore have represented contamination or re-infection from in-contact cats in the other treatment groups that were still shedding organisms.
Duration of C psittaci shedding in the four treatment groups

Cats still shedding C psittaci at the end of the study (day 35).
Discussion
Active infection with typical signs of experimentally-induced feline chlamydiosis were induced in all cats used for this study (Hoover et al 1978, Wills et al 1986, O'Dair et al 1994). Treatment was delayed until day 7 to allow overt clinical disease to develop in all the cats, thus mimicking therapy in a clinical setting.
The results from this study showed that following therapy, the doxycycline-treated group had consistently the lowest median clinical scores (with the exception of day 35) and that this was significantly different from the placebo treatment within just 24 h of commencement of therapy. Although significant differences were mainly documented between the placebo and doxycycline treatments, a clear trend emerged in the clinical scores of the four groups, with little observable difference between the fusidic acid and placebo-treated groups, but the chlortetracycline-treated group lying between the placebo and doxycycline-treated groups. The changes in the clinical scores were also reflected by the changes in isolation of C psittaci from the cats, with the median duration of shedding of the organism being shortest in the doxycycline-treated group and longest in the placebo and fusidic acid-treated groups. We used culture of conjunctival swabs to identify viable C psittaci organisms during this study. Recently, polymerase chain reaction (PCR) techniques have been developed for detection of feline C psittaci, which can be more sensitive than in vitro culture (McDonald et al 1998). However, culture has the advantage of only detecting viable organisms, whereas PCR may also detect non-viable genetic material (McDonald et al 1998).
These results clearly demonstrated systemic (doxycycline) therapy had superior efficacy to topical (chlortetracycline) therapy under the conditions of this study. Furthermore, we found no evidence that topical fusidic acid alone had any efficacy in the treatment of feline chlamydiosis, both by comparing groups P and F, and by comparing group D with our previous experience of using doxycycline alone for the treatment of experimentally-induced chlamydiosis (Sturgess et al 1996, Sturgess CP—unpublished observations). Nevertheless, although topical fusidic acid did not affect the course of clinical disease in these cats, it is possible that the addition of a topical agent that provides ophthalmic lubrication may help to reduce any local discomfort associated with the disease.
For logistical reasons, we only administered topical therapy twice daily in this study. Although twice-daily application is within the current data sheet recommendations for the use of chlortetracycline ophthalmic ointment, it is quite possible that this therapy might have produced an enhanced effect if more frequent applications had been given. Nevertheless, restriction to two or three daily treatments is common in clinical practice, and even if more frequent application were feasible, it seems improbable that the clinical efficacy would exceed that demonstrated with single daily oral dosing of doxycycline in this study. However, further specific studies would be required to investigate this.
In addition to the superior efficacy demonstrated by systemic therapy in this study, another reason for not relying on topical therapy alone for the treatment of feline chlamydiosis is the potential existence of the organism at extraocular sites. Chlamydia psittaci has been routinely isolated from both vaginal and rectal swabs in cats experimentally-infected with the organism (Wills et al 1987, O'Dair et al 1994), and there is also evidence of the organism infecting the gastric mucosa of naturally-exposed cats (Gaillard et al 1984, Hargis et al 1983). It has been suggested (Gaillard et al 1984) that the mucosa of the gastrointestinal tract may act as a reservoir for chlamydia, and if so, systemic therapy would clearly be preferable in the hope of eliminating this reservoir in addition to the ocular infection. However, this aspect was not specifically evaluated in the current study.
In conclusion, this study has demonstrated that both topical chlortetracycline and systemic doxycycline are effective therapeutic agents for feline ocular chlamydiosis. However, systemic doxycycline produced a more rapid clinical and microbiological resolution of disease and, based on these results, would be the preferred treatment unless systemic therapy was contra-indicated.
Footnotes
Acknowledgements
AH Sparkes was supported by the Feline Advisory Bureau. This study was supported by a grant from Leo Laboratories Ltd.