
Abstract
Background
Ellis–van Creveld is a dwarfing syndrome transmitted as an autosomal recessive trait. The constant features of the condition include acromelic–micromelic dwarfism, ectodermal dysplasia involving the nails, teeth and gums, postaxial polydactyly of the hands and congenital heart disease. Congenital heart disease affects 50–60 % of all patients and nearly 50 % of patients die by 18 months of age from cardiopulmonary complications. This study is intended to characterise the orthopaedic manifestations of Ellis–van Creveld based on the authors’ unique opportunity to interview and examine the largest group of patients to date in the literature.
Methods
Detailed interviews, physical examinations and/or radiographs were available on 71 cases of Ellis–van Creveld syndrome. Data were collected from physical examinations, radiographs, computed tomography (CT) reconstruction and magnetic resonance imaging (MRI) of the knee. Pathoanatomy of the knee was reinforced by the direct surgical observation of 25 limbs surgically managed during adolescence and puberty.
Results
A number of interesting clinical and radiographic abnormalities were noted in the upper extremities and lower extremities, but by far the most significant orthopaedic finding was a severe and relentlessly progressive valgus deformity of the knee. Although many patients had difficulties making a “fist” with the hand, no patient reported any functional disability. The severe valgus deformity of the knee is the result of a combination of profound contractures of the iliotibial band, lateral quadriceps, lateral hamstrings and lateral collateral ligament, leading to lateral patellar subluxation and dislocation. The lateral portion of the upper tibial plateau presents with cupping and progressive depression of the lateral plateau, along with severe valgus angulation of the proximal tibia and fibula. A proximal medial tibial exostosis is seen in nearly all cases.
Conclusion
This is the largest group of Ellis–van Creveld syndrome patients identified in the literature. An understanding of the orthopaedic pathoanatomy of the knee deformity is critical to determining the appropriate surgical management. This paper characterises the orthopaedic manifestations of Ellis–van Creveld syndrome and especially identifies the pathoanatomy of the severe and progressive valgus knee deformity.
Level of evidence
Level II.
Introduction
Chondroectodermal dysplasia (Ellis–van Creveld syndrome) is a very rare form of skeletal dysplasia seen most commonly in, but not limited to, the Old Order Amish population. It is estimated that <300 cases have been reported in the English-speaking literature. In 1964, McKusick et al. [1, 2] reported 52 cases in the Old Order Amish (of whom 30 died within the first year of life), the largest single group of affected patients reported at that time, and established the genetic transmission as autosomal recessive [3–6]. Others have suggested the transmission as autosomal recessive [7–9]. The origins of this disorder and its particular pedigree were traced to one Samuel King and his wife, who emigrated from Europe in 1744. Recently, the genes which when mutated produce the condition have been identified [10–14]. The focus of the mutant gene is at 4p16 and represents mutations in two separate EVC genes, EVC and EVC2. The incidence has been estimated at 0.9 cases per 100,000 live births [6]. The genes EVC and EVC2 are highly expressed in bone and heart, two organs predictably affected in individuals with Ellis–van Creveld syndrome. Recent evidence suggests that EVC genes are involved in bone growth mediated at the base of primary cilia [15].
In 1670, Kerckring [16] reported a case of a polydactylous dwarf found drown in a river that might have represented one of the earliest cases ever reported of this condition. The infant had seven fingers and nine toes on one side and seven fingers and seven toes on the other. The drawing from the publication suggests a mesomelic form of dwarfism. Unfortunately, the absence of soft tissue findings renders the case speculative at best. In 1933, McIntosh [17] reported what is currently accepted as the first case reported in the modern literature of Ellis–van Creveld syndrome. In 1940, paediatricians Richard Ellis and Simon van Creveld [18] fully clarified the condition, alluding to the 4.5-year-old case described by McIntosh, and have subsequently received eponymous recognition of the condition. Small numbers of cases of Ellis–van Creveld have been reported in many races and in a multitude of countries throughout the world [19–45]. Currently, the Amish population of eastern Pennsylvania (primarily Lancaster County) still contains the largest concentration of patients with this condition in North America and, likely, outside of North America. Prenatal diagnosis by ultrasound is available [26–49].
The existing literature, albeit assembled from a relatively large number of publications of a small number of patients, paints a picture of a core group of consistent findings that characterise the syndrome across all patients and a larger constellation of findings frequently encountered in many patients but absent or incompletely expressed in others [50–59]. In 1973, Bailey [60] provided a useful overview of the many associated features. A few other clinical findings are only occasionally encountered. The most consistent and typical components of Ellis–van Creveld syndrome include acromelic–micromelic chondrodystrophic dwarfism and ectodermal dysplasia involving the nails, teeth and gums; postaxial polydactyly of the hands and occasionally of the feet; and commonly but not consistent congenital heart disease involving variable defects, most often a single atrium with cleft mitral valves (50–60 % of all patients). The usual average adult height is between 43 and 60 inches (110 and 152 cm.) It has been estimated that nearly a third of the patients die in the first 6 months and up to a half by 18 months of age from cardiac or pulmonary consequences.
A recent, unique opportunity to interview and examine a sizeable group of Amish patients with Ellis–van Creveld syndrome and a few non-Amish cases has prompted an assessment of the orthopaedic manifestations of this condition. Furthermore, an opportunity to directly surgically observe the pathoanatomy of the profound and severe valgus deformity of the knee has provided documentation of the nature of the marked extensive soft tissue contractures and chondro-osseous deformity seen in this condition.
Material—data
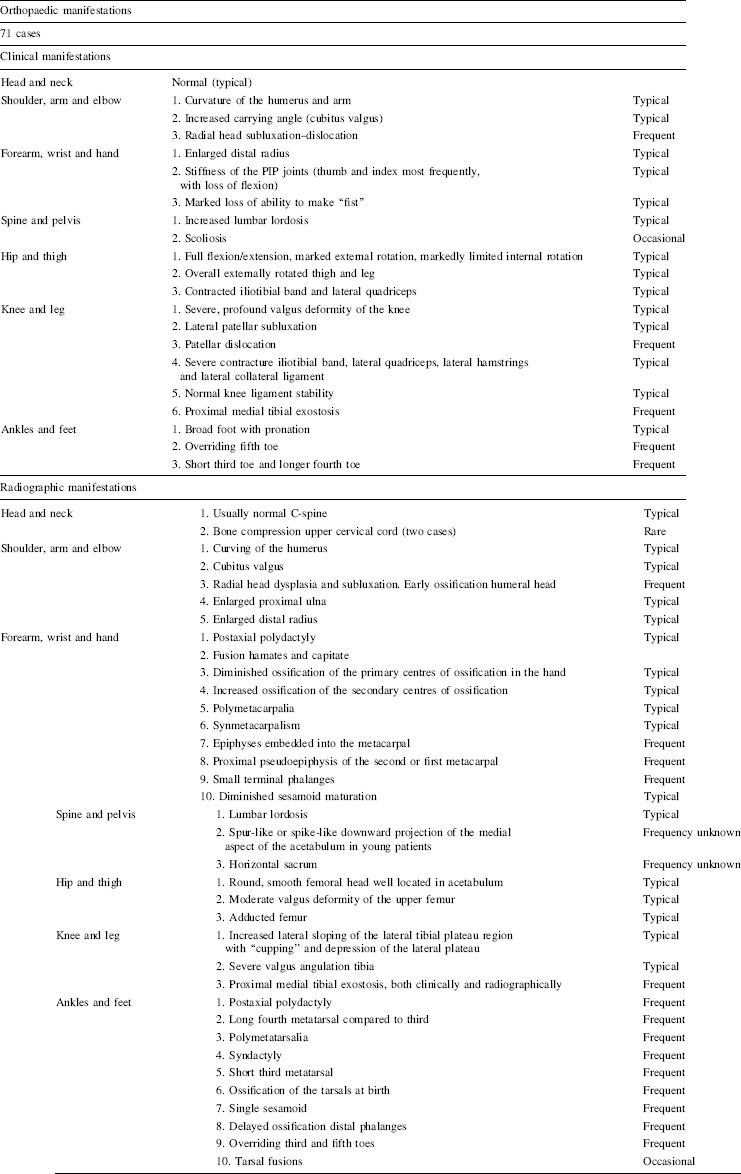
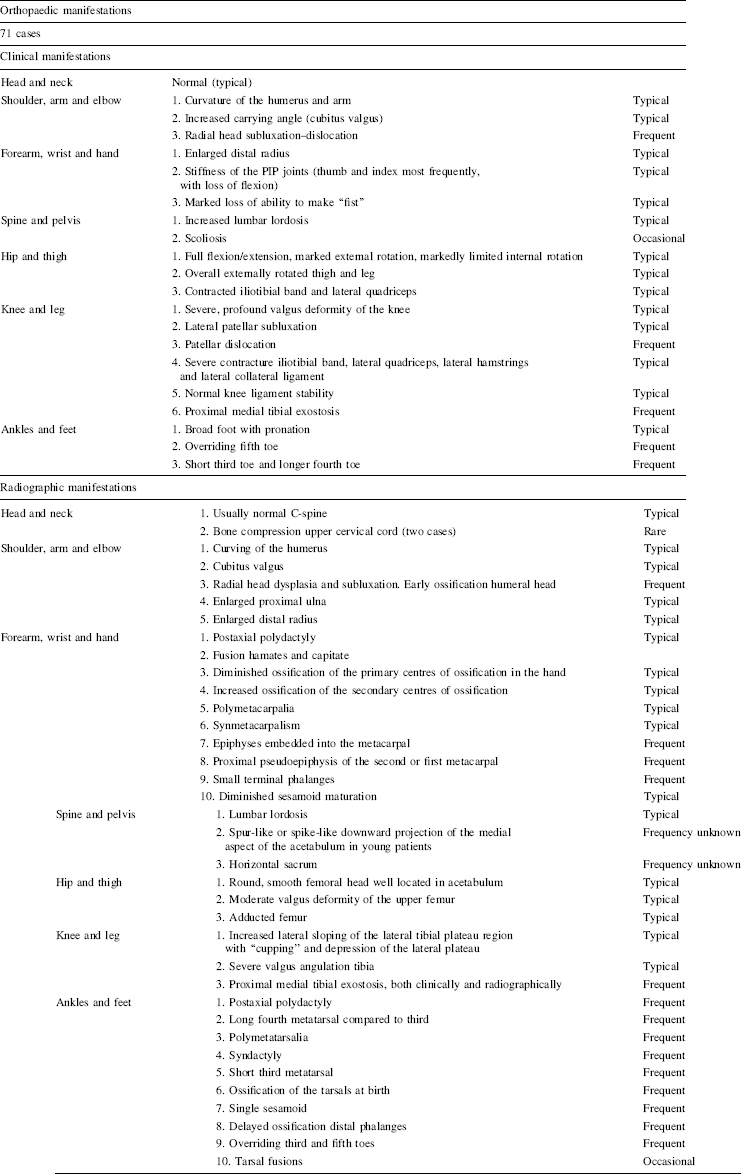
General clinical and radiographic characteristics of Ellis–van Creveld syndrome
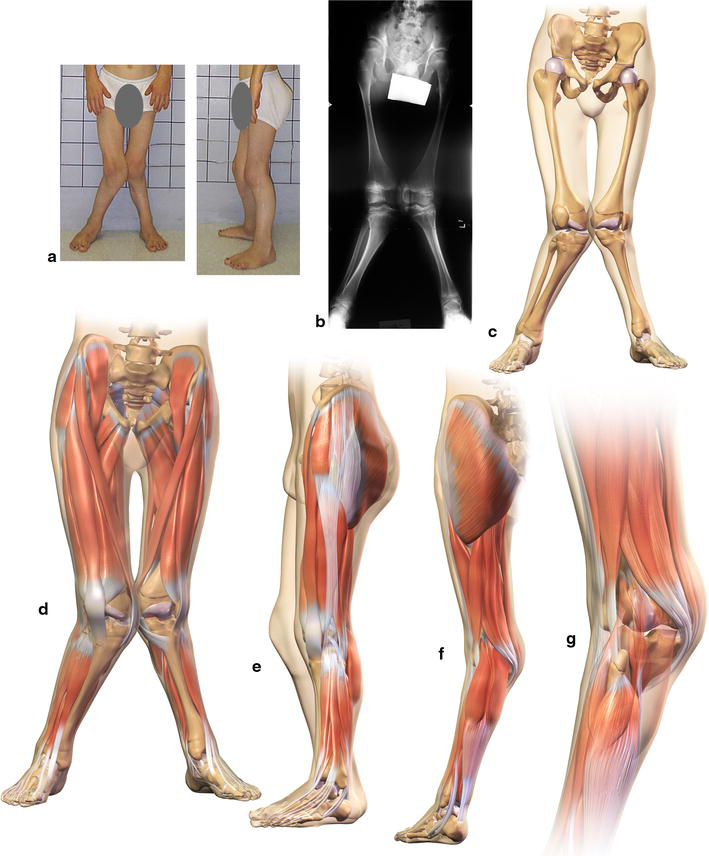
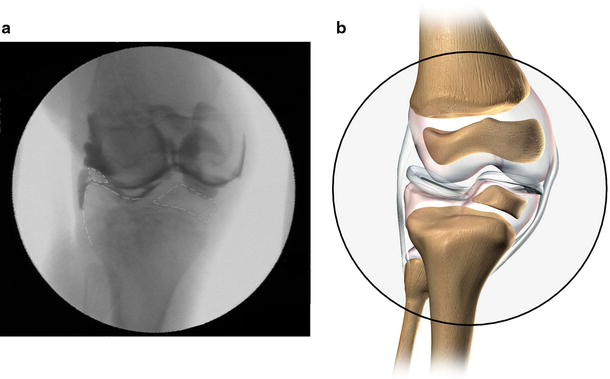
Approval from our institutional review board was obtained. Detailed interviews, physical examinations and/or radiographs were available on all 71 patients included in this study. All but three of the patients descended from Old Order Amish backgrounds. Radiographic evaluations were available on 47 patients; 80 lower extremities; 31 skeletal surveys, including upper extremities and spine; 13 computed tomography (CT) reconstructions of the knee; and four magnetic resonance imaging (MRI) scans of the knee. Radiographs of the knee were available on all patients, not surprisingly, inasmuch as the knee valgus deformity is the most obvious and functionally impairing deformity routinely seen in Ellis–van Creveld syndrome (Fig. 1a–g). Online Resource 1 depicts a rotating 3-D computer model of Fig. 1 showing severe genu valgum, cupping of the lateral tibial plateau and patellar dislocation of the left knee.
The hair may be sparse or absent or fine and silky. Teeth may be present at birth with wide-spaced, peg-shaped hypoplastic teeth or even absent teeth. The gums are usually serrated and the upper lip is commonly attached to the upper gum in the form of a partial pseudocleft resembling a harelip but clearly different anatomically. Intelligence is generally normal or just slightly below. The nails are usually described as dystrophic, fragile, fluted and bordered by a peculiar brown rim. Dysplastic nails are seen uniformly in all patients.
For the purpose of this paper, we have arbitrarily divided the manifestations into typical (over 90 % of cases), frequent (50 % or more) and occasional (<50 % of cases).
Surgical observations (14 patients, 25 limbs)
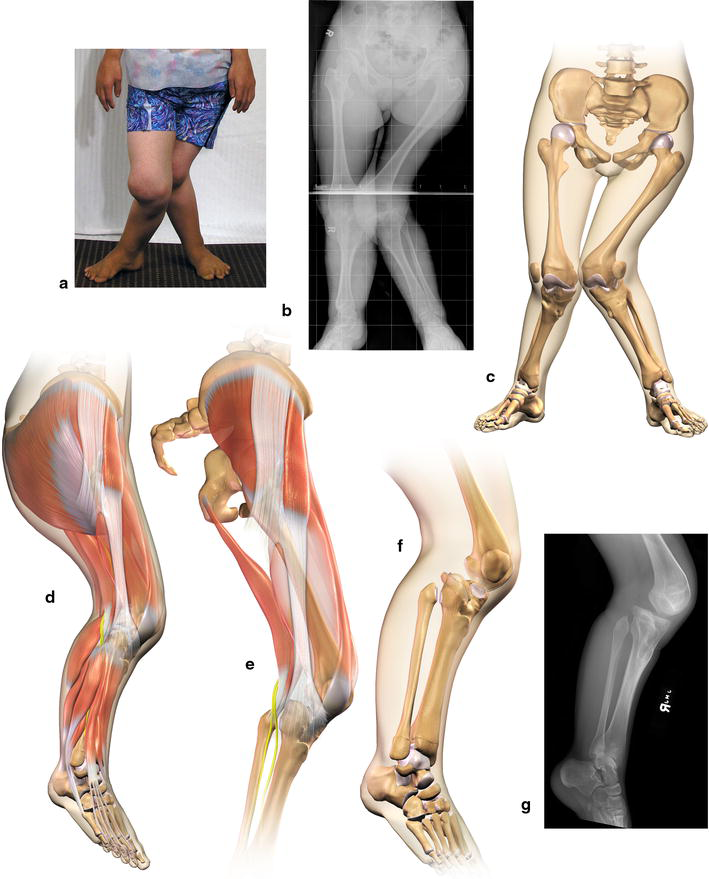
On the basis of direct surgical observation in an attempt to correct the severe valgus deformity of the knee, the following observations were routinely encountered in all cases to varying degrees. In 25 consecutive cases in the 10- to 16-year-old age group of patients, the following findings were typical (Figs. 1, 2 and 3; Online Resource 2 depicts the severe osseous pathoanatomy in a rotating 3-D computer model of Fig. 2, whereas Online Resource 3 includes the accompanying soft tissue abnormalities in a 3-D rotating rendition):
Lateral subluxation or dislocation of the patella. Severe contracture of the iliotibial band, vastus lateralis and the lateral retinaculum, and capsule of the joint. Contracture of the lateral hamstrings. Contracture of the lateral collateral ligament. Valgus lateralization and insertion of the infrapatellar tendon. Deep “saucer”-like depression of the lateral tibial plateau. Severe valgus of the shaft of the tibia, particularly proximally. Medial proximal tibial exostosis.
Although the ankle and foot are in pronation and the metatarsals and toes have frequent angular and rotation deformities, not a single patient had any foot or ankle complaint that led to any surgical correction. An unexplained and interesting observation in this group of patients was the frequency of delayed independent walking. Data were available on 43 of 71 patients who walked independently at an average of >15 months (range 11–35 months). The reason for this finding currently remains unclear.
Discussion
Although clinical and radiographic findings were often interesting and abnormal, the abnormalities surprisingly did not produce any functional limitations in the upper extremity, except the inability to produce a “fist” that was mentioned only rarely by an occasional patient on direct questioning, in spite of routinely encountered stiffness in the interphalangeal joints.
Significant restriction of flexion of the proximal interphalangeal (PIP) joints of the hand, often the thumb and index fingers, was seen very frequently (Fig. 4). One would presume that this restriction would result in the impairment of fine motor skills necessary in many occupations in society. The PIP joint stiffness is likely less impairing in the Amish due to occupational types. In the Amish society, nearly 70 % of males are employed in farming and roughly 30 % in construction and repair trades, such as carpentry, cabinet making, blacksmithing and harness repair or as labourers on farms and construction sites [61]. Unmarried Amish girls often work as store clerks or maids and only rarely work outside the house after marriage [61].

X-rays—upper extremity radiographic changes
Recent identification of two cases of upper cervical bony cord compression is, at the very least, distressing, but it is unclear whether the bony compression is directly related to the EVC syndrome. Routine lateral flexion/extension radiographs or other more detailed radiographic imaging of the upper cervical spine and base of the skull has not been suggested in the past. These cases warrant an increased awareness at least of the possible linkage to the basic condition in rare cases.
The thoracolumbar spine is usually spared deformity, save for an increased lumbar lordosis, which is seen frequently (Fig. 5). Scoliosis is seen only occasionally and kyphosis has not been seen at all in this group of patients or reported to be related to the syndrome. The fascinating radiographic changes in the acetabulum seen early in patients with Ellis–van Creveld (medial spike-like osseous prolongation) [62–65] appear to disappear with progressive osseous maturation, as the changes are not seen in skeletally mature individuals with Ellis–van Creveld syndrome, nor do they result in acetabular dysplasia.

X-ray—lateral spine
The femoral head is round, smooth and routinely well positioned in the acetabulum, with the head, neck and proximal shaft positioned in a valgus alignment. The femoral shaft is usually adducted and the overall bony alignment of the head–neck shaft is in moderate valgus. The marked contracture of the iliotibial band and lateral quadriceps, with significant external rotation of the thigh musculature, likely results in the marked clinical external rotation of the hip relative to very limited internal rotation of the hip and was present in nearly all patients. The common peroneal nerve remains adherent to the biceps tendon and is pulled away from its normal course around the neck of the fibula (Fig. 2e), all of which are demonstrated in the rotating 3-D modelling in Online Resource 3.
The soft tissue contractures likely contribute to the bony valgus and external rotation of the femur as well. Flexion/extension ranges of motion of the hip were normal. The severe soft tissue contracture of the iliotibial band and quadriceps is most reflected at the knee level (Figs. 1e and 2e).
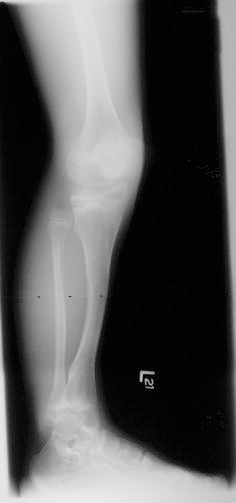
Without question, the most striking and functionally impairing orthopaedic deformity affecting patients with Ellis–van Creveld is the severe and relentlessly progressive valgus deformity of the knee. This progressive valgus results in diminished efficiency in ambulation, with increased energy expenditure, and, in some cases, the inability to maintain ambulation. The extent of the valgus angulations far exceeds that seen by the authors in any other known orthopaedic condition. Thigh–leg angulations over 45° were routinely seen, with the lower extremities crossing over each other during ambulation, as shown in Online Resource 4, which is a gait video of a preoperative Ellis–van Creveld patient.
The peculiar lateral sloping and “cupping” and depression of the lateral tibial plateau was present in all cases [1, 7, 60–73], seen before walking age and progressively increased in dimension thereafter. In addition, the proximal lateral tibial plateau slopes in a variable fashion either laterally forward or, to a lesser extent, posteriorly from one patient to another, or even between the right and left knees of the same patient (Figs. 6 and 7). Ironically, the medial aspect of the knee joint remains well formed and intact, forming a pivot point against which the tibia may rotate externally or, in some cases, internally, corresponding with the degree of flexion deformity or recurvatum of the knee. Online Resource 5 demonstrates a computer modelling of Fig. 1, morphing between the right and left knees, depicting the variable slope of the lateral plateau, corresponding with flexion deformity and recurvatum, respectively. The medial aspect of the knee joint remains well formed and intact, forming a pivot point against which the tibia may rotate externally or, in some cases, internally. In severe cases, the lateral tibial plateau may sublux posteriorly, exacerbating the knee valgus (Fig. 2c, f), as demonstrated in Online Resource 3. The defect is believed to be a primary bony dysplasia and an inherent component of Ellis–van Creveld syndrome. Secondary weight-bearing changes likely augment the deformity and increase the valgus (Fig. 3). Online Resource 6 provides a conceptual morphing model between normal to a 13-year-old Ellis–van Creveld patient, depicting secondary weight-bearing changes. A proximal medial tibial exostosis (osteochondroma) is seen in most cases. Although speculative at best, it may occur secondary to “traction” on the physis by the relentlessly progressive valgus deformation of the tibia.
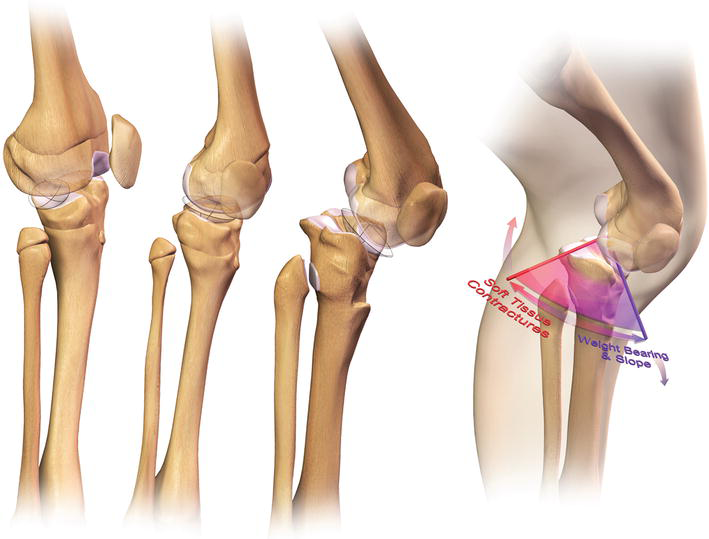
Illustration of the variable lateral tibial plateau defect
X-ray—lateral knee and ankle
The profound soft tissue contracture of the iliotibial band, the lateral quadriceps, the lateral hamstrings and the lateral collateral ligament results in progressive lateral displacement of the patella, with eventual subluxation and dislocation. These soft tissue contractures “tether” the tibia and fibula into further valgus (Fig. 2e). The authors believe that the soft tissue contracture is every bit as important in producing the severe overall valgus as the bone deformity. The failure of most isolated bony surgical attempts at correction substantiates the role of the soft tissue contracture aetiologically [74–79]. Currently, the authors have no plausible explanation for the delay in independent walking frequently seen.
Conclusion
Although a myriad of clinical and radiographic orthopaedic abnormalities have been identified in association with the Ellis–van Creveld syndrome, the severe knee valgus deformity is the only one to produce significant orthopaedic impairment and disability. Recognition of the soft tissue and bony pathoanatomy of the knee is essential to avoid fruitless surgical attempts at correction.
Footnotes
Acknowledgements
The authors wish to express their appreciation to Richard Pauli, M.D. for providing access to two non-Amish patients’ information and to the Women's Board of Akron Children's Hospital for the research funding support.
No direct or indirect commercial financial incentive was associated with this publication. This study was supported in part by a grant from the Women's Board of Akron Children's Hospital. The authors declare no conflict of interest.