
Abstract
Abstract
There is growing evidence that symptomatic femoroacetabular impingement leads to intra-articular damage and the development of early-onset osteoarthritis. Symptoms of femoroacetabular impingement often do not manifest until adulthood, but have been increasingly recognised in the paediatric and adolescent population. The surgical treatment of femoroacetabular impingement is aimed at restoring a more normal femoral head–neck offset in order to increase the clearance and prevent femoral abutment against the acetabular edge. Current methods include open and arthroscopic techniques. The latter has been combined with an open approach to gain access to the head–neck junction for osteochondroplasty. Proximal femoral and/or periacetabular osteotomies are used to treat femoroacetabular impingement associated with deformity secondary to childhood hip conditions, such as slipped capital femoral epiphysis and Legg–Calvé–Perthes disease. Some adolescents have severe degenerative joint disease at the time of presentation and may require arthroplasty or arthrodesis. The aim of this review is to identify the major trends and advancements in the management of femoroacetabular impingement in adolescents, including the outcome of studies of the surgical treatment modalities used.
Introduction
There is growing evidence that symptomatic femoroacetabular impingement (FAI) leads to progressive intra-articular damage and the development of early-onset osteoarthritis (OA) if left untreated [1]. FAI results from pathological contact between the femoral head and the acetabular rim due to either an abnormal femoral head–neck junction (cam lesion) and/or excessive anterolateral coverage of the femoral head (pincer lesion) or a combination of both [2]. Symptoms of FAI are becoming increasingly recognised in the paediatric and adolescent population [2, 3].
The surgical management of FAI is aimed at correcting the impingement morphology while restoring a more normal femoral head–neck offset in order to increase the clearance and prevent femoral abutment against the acetabular edge. Open, arthroscopic and combined treatment methods used in adult patients have been successfully applied to paediatric and adolescent patients [2–14].
The aim of this review is to identify the major trends and advancements in the management of FAI in adolescents and provide a balanced approach involving the various surgical treatment modalities to treat the condition.
Aetiology of FAI
Based on the type of underlying abnormal morphology, FAI can be characterised into three types: cam, pincer and mixed-type impingement [1]. In cam-type impingement, the relative prominent area typically on the anterolateral femoral neck, due to reduced femoral head–neck offset, abuts the acetabular rim during forceful motion, especially in flexion and internal rotation, leading to damage of the labral-chondral complex [15]. This abnormal contact exposes the acetabular labrum and acetabular cartilage to outside-in shear forces at the anterosuperior rim region [1]. In pincer-type impingement, the structural abnormality is on the acetabular side, involving focal or global overcoverage of the femoral head, leading to impaction damage of the femoral head–neck region and labral damage as well [16–18].
In many cases of adolescent FAI, the underlying structural abnormality is secondary to residual deformity from the sequelae of childhood hip diseases such as Legg–Calvé–Perthes disease (LCPD) and slipped capital femoral epiphyses (SCFE) [19–21]. Iatrogenic causes, particularly post-surgical following overenthusiastic pelvic osteotomies such as single innominate, triple or periacetabular osteotomy (PAO) of the pelvis, can sometimes lead to retroversion of the acetabulum due to overcorrection, leading to pincer-type impingement [22]. It is important to note that some of these childhood osteotomies do remodel with time and may no longer have impingement morphology after the growing years [23]. However, in most cases, there is no history of previous hip pathology and FAI may, therefore, be considered to be primary or idiopathic [3].
Primary FAI
Morphological abnormality seen in primary cam-type impingement is similar to the deformity seen in SCFE and LCPD; therefore, Ganz et al. [24] suggested that these conditions may have occurred sub-clinically during development. It has also been proposed that the cam-type lesion occurs as a result of abnormal bone growth from the epiphysis [25].
Genetic influences have been implicated in the development of primary FAI [26]. Pollard et al. [26] screened 96 siblings of 64 patients with primary FAI clinically and radiologically for the presence of cam and pincer lesions and showed that the siblings of patients with a cam deformity and a pincer deformity had a relative risk ratio of 2.8 and 2.0 of having the same deformity, respectively. It is unclear as to whether the genetic component determines the deformity at conception or if it predisposes to abnormal development or sub-clinical hip pathology before skeletal maturity.
Siebenrock et al. [27] recently published their observations, suggesting that a high intensity of sports activity during adolescence is associated with a substantial increase in the risk of cam-type impingement. These patients may also be at increased risk of subsequent development of secondary coxarthrosis.
Secondary FAI
SCFE
In SCFE, the relative positioning of the femoral head leads to prominence of the anterolateral femoral metaphysis (Fig. 1) [28, 29]. This leads to cam-type impingement and subsequent wear of the labrum and acetabular cartilage. The severity of the slip correlates with poor long-term clinical outcome scores and radiographic evidence of OA [30]. Even cases of mild slip that have had in-situ pinning in the past can develop symptomatic FAI with time [31].

AP pelvis radiograph showing post-SCFE secondary cam deformity of the right hip
Rab studied the implication of SCFE geometry on impingement, describing two different mechanisms that lead to damage of the labral-chondral complex, impaction and inclusion [32]. In the impaction-type mechanism, the abnormal contact between the prominent femoral metaphysis and the acetabular rim results in damage to the labrum. With increased flexion, the femoral head may lever out of the acetabulum and cause contre-coup acetabular articular cartilage damage. The metaphyseal prominence can fall within the acetabulum in low-grade SCFE or following remodelling of the metaphysis. The included portion can produce outside-in abrasion to the acetabular cartilage [28].
LCPD
Residual deformity in LCPD may cause hip pain in adolescents and young adults, owing to altered hip joint biomechanics [33]. Contributory factors include abnormal femoral head shape, disturbance of the proximal femoral physis and acetabular dysplasia due to remodelling. Symptoms may be related to hip joint instability, FAI or a combination [34]. Causes of FAI in LCPD include the aspherical femoral head, acetabular retroversion or secondary deformity following surgical procedures such as innominate osteotomy [31, 33–35]. These can lead to intra-articular impingement, but extra-articular impingement can also result from overgrowth of the greater trochanter or, less commonly, the lesser trochanter due to shortening of the femoral neck [34].
The majority of studies on the progression of deformity in children in SCFE and LCPD have focussed on the proximal femur, but a number of studies have demonstrated that FAI can occur in both conditions as a result of acetabular retroversion [36, 37]. Sankar and Flynn [37] have found that acetabular retroversion was rare in children with LCPD before skeletal maturity, but increased significantly around maturity.
Others
Other causes of secondary FAI include previous fractures of the proximal femur and hereditary multiple exostoses [5, 38].
Clinical and radiological evaluation of FAI
FAI typically affects active young adults who usually complain of slow-onset groin pain, which is initially intermittent, precipitated by excessive demand on the joint, such as during sporting activities. It may also be related to flexion activities like prolonged sitting and squatting. A history of true locking or catching sensation in the hip can be elicited if there is an underlying intra-articular mechanical problem, such as labral tear or chondral flap, which can be associated with FAI.
There are specific physical findings in patients with FAI. Anterior FAI is more common than posterior FAI, where the femoral neck abuts against the anterior acetabulum and the labrum when the hip is flexed and internally rotated, producing deep-seated groin pain. Posterior FAI occurs with the hip in extension and external rotation. An impingement test is performed with the patient supine and the hip is internally rotated as it is passively flexed to around 90° and adducted. This test is almost always positive in anterior FAI [16]. The clinical test for posterior FAI is, again, done with the patient supine, but with the affected leg hanging from the end of the bed in order to produce maximal extension. The test is positive if pain is produced on external rotation of the extended leg.
Investigations often used for FAI consist of combinations of magnetic resonance imaging (MRI), computed tomography (CT) and plain radiographs. MRI can detect labral pathology, as well as the condition and extent of coverage of cartilage of the femoral head. The use of CT scanning allows direct measurement of the acetabular version [39].
On the AP view of the pelvis, there are three signs which suggest abnormality of the acetabulum related to FAI: the posterior wall sign, the crossover sign and the ischial spine sign. Normally, the lines representing the anterior and posterior wall of the acetabulum meet at the lateral edge of the acetabulum on the AP view; however, if the acetabulum is retroverted, they are seen to cross over each other (the crossover sign). The posterior wall sign is when the posterior wall line is projected medial to the centre of the femoral head. The ischial spine, which is not normally visible on the AP view, becomes visible in acetabular retroversion (the ischial spine sign). It is extremely important to get an accurate position of the AP view, as the position of the centre of the beam, pelvic tilt and rotation can affect the three signs of retroversion [40].
The AP pelvic view may reveal a flattened femoral head or a pistol grip deformity, both of which are associated with cam lesion. An alpha angle is a parameter used to quantify the degree of femoral head deformity and can be measured on the lateral view of the proximal femur. This is the angle between the longitudinal axis of the femoral neck and a line connecting the centre of the femoral head with the point where the femoral head loses its sphericity [41]. The normal alpha angle for men is 68° or less and, for women, it is 50° or less [42]. A greater angle suggests abnormal femoral head–neck contour.
Treatment of FAI
Non-operative management
A trial of non-operative management, including activity modification and non-steroidal anti-inflammatory drugs (NSAIDs), may have some role in controlling symptoms. Emara et al. [43] followed up patients with FAI with alpha angles less than 60° managed conservatively through activity modification for 24 months. They found that non-operative treatment was effective in improving function and symptoms, although no improvement in the range of motion (ROM) was noted. Whether these symptoms returned is not known, as no longer follow-up was reported.
However, adolescent patients with idiopathic FAI typically have high activity levels and athletic ambitions that make non-operative management only successful temporarily [16]. Patients treated in this manner should be followed up closely, as continued impingement can lead to the progression of damage to the labral-chondral complex and subsequent development of OA [44].
Operative management
The surgical treatment of symptomatic FAI is focussed on correcting the impingement morphology, thereby, improving hip motion and alleviating symptoms and delaying the progression towards early OA.
Surgical intervention can be accomplished in various ways:
Open surgical techniques involving safe surgical dislocation of the femoral head, with additional intervention, including femoral or pelvic osteotomies (PAO), as deemed necessary on a case-to-case basis. Mini-open methods that do not involve a trochanteric flip osteotomy and a complete surgical dislocation. These techniques may involve arthroscopic assistance as well. Arthroscopic methods only for treatment.
There is no consensus defining the indication for different types of intervention in the treatment of FAI; therefore, whether the surgery is performed openly or arthroscopically is more a reflection on the individual surgeon's experience and comfort with various procedures. However, if the deformity underlying the FAI is severe, such as those associated with LCPD or SCFE, an open approach may be more appropriate, as it allows procedures like proximal femoral osteotomy and periacetabular osteotomy to be performed in conjugation with the osteochondroplasty, as the latter alone may be insufficient to permit impingement-free ROM.
Surgical dislocation and osteochondroplasty (SDO)
Ganz et al. [45] described a technique of safe surgical hip joint dislocation, which protects femoral head vascularity, for the treatment of intra-articular hip pathology in adults. They reported no osteonecrosis in a series of 213 patients undergoing surgical hip dislocation using this technique. The technique has been successfully applied to paediatric and adolescent patients [6, 11, 46, 47].
Outcome of SDO in adolescents
There are no studies on the outcome of SDO in the treatment of FAI in a purely adolescent population; however, there are three mixed studies available [6, 11, 14].
Peters and Erickson [6] treated 30 hips (in 29 patients; mean age 31 years) using the surgical dislocation technique described and debridement with or without relative femoral neck lengthening and a minimum follow-up of 2 years. The specific diagnoses were primary FAI in 25 patients, LCPD in three patients and SCFE in one patient. The mean Harris hip score (HHS) improved from 70 pre-operatively to 87 at final follow-up. None of the patients developed osteonecrosis or trochanteric non-union, but there were three cases of conversion to total hip replacement due to pain and/or progressive arthrosis. All three patients had grade IV acetabular cartilage damage and the authors emphasised the need for better imaging methods to assess the articular damage. Similar improvement in HHS was noted in another study by Peters et al. [14]. Naal et al. [11] assessed the outcome of SDO in 22 male professional athletes and reported that 21 of the 22 patients returned to compete professionally, with the majority being happy with their sporting ability.
Hip arthroscopy
Hip arthroscopy offers a less invasive technique for the diagnostic and therapeutic management of FAI in good hands [48–51]. The potential advantages of arthroscopy over open surgery include lower morbidity, less recovery time, earlier return to full activity and the avoidance of a complete hip dislocation, with less intra-operative blood loss [52, 53].
Combined hip arthroscopy with limited open osteochondroplasty
Hip arthroscopy has been carried out in combination with an open osteochondroplasty via a mini-anterior approach [5, 8]. Arthroscopy is first carried out to inspect the joint as well as to treat labral and chondral pathology. An 8–10-cm incision made along the Smith–Peterson interval (which is more cosmetically appealing if made as a bikini-line incision) is utilised to expose the anterolateral femoral head–neck junction and the anterosuperior acetabular rim [5]. Clohisy et al. [5] argued that combining arthroscopy with an open approach allows better exposure of the femoral head–neck junction and less potential for osseous debris entrapment in the joint compared to arthroscopy alone. Resection of the cam lesion under direct vision minimised the risk of inadequate correction. Although this technique will not allow circumferential lesion of the femoral head or acetabulum to be treated, it may be appropriate for FAI, which is localised mainly anteriorly.
Outcome of arthroscopic treatment
We identified six case series [3, 4, 7, 9, 12, 13], two of which monitored the outcome in purely adolescent [3, 12] and the rest in mixed adolescent and adult patients. Five studies reported improvement in the mean modified HHS (MHHS) post-operatively. One study did not use any scoring system, but reported that 93 % of athletes returned to professional competition after surgery [4]. Larson and Giveans [7] performed impingement testing pre- and post-operatively. All patients tested positive for the test pre-operatively and this reduced to 14 % following arthroscopic treatment (p < 0.001). The reported post-operative complications included transient sciatic neurapraxia, heterotopic ossification and adhesion. Larson and Giveans [7] reported three patients who underwent total hip replacement at their most recent follow-up, but all were noted to have grade IV chondral damage at the time of arthroscopy. Haviv and O'Donnell [13] studied the clinical outcome in 82 patients presenting with bilateral cam-type FAI undergoing sequential bilateral arthroscopic femoral osteochondroplasties. The mean MHHS and non-arthritic hip score (NAHS) improved significantly in both hips following arthroscopic osteochondroplasty (p < 0.05).
Outcome of arthroscopic treatment combined with limited open osteochondroplasty
Laude et al. [8] monitored the outcome of 97 patients undergoing osteochondroplasty using a mini-anterior approach with arthroscopic assistance. The result was promising, with an increase in the average NAHS by 29.1 at a mean follow-up of 28.6 months. However, there was a case of femoral neck fracture 3 weeks post-operatively. In another study, 35 patients were treated for FAI using the combined approach [5]. The average MHHS improved from 63.8 points pre-operatively to 87.4 points at the time of last follow-up. Minor complications, such as superficial wound infection, deep vein thrombosis and asymptomatic heterotopic ossification, were noted.
Table 1 shows a summary of the studies mentioned above.
Denotes pure paediatric/adolescent study
Outcome following arthroscopic osteochondroplasty of one hip is shown. Groups 1 (n = 45) and 2 (n = 37) consist of patients presenting with bilateral symptoms and unilateral symptoms, respectively
Treatment of secondary FAI
SCFE
In a case of chronic SCFE with symptomatic FAI, proximal femoral osteotomy (PFO) can be performed in the sub-trochanteric, inter-trochanteric, basi-cervical or sub-capital region in order to help restore the morphology of the proximal femur while addressing the component of intra-articular FAI. Fixation is commonly internal, although some studies have attempted external fixation with good results [54, 55].
The more proximal the osteotomy (i.e. basi-cervical and sub-capital), the greater the potential for correction of chronic slip deformity in SCFE [56]; however, there is an increased risk of osteonecrosis and chondrolysis [57]. For example, osteonecrosis has been reported to occur at a rate of 10–100 % [58–60].
Inter-trochanteric osteotomy creates flexion, internal rotation and valgus at the osteotomy site and is used to reduce the femoral head–neck offset responsible for impingement [61]. The Imhäuser corrective osteotomy is performed just proximal to the lesser trochanter perpendicular to the femoral shaft [56, 61]. A bone wedge from the proximal fragment can be removed to create flexion at the osteotomy site or an end-to-side apposition of the osteotomy can be performed, where the anterior cortex of the proximal fragment is impacted into the medullary canal of the femoral shaft [61, 62]. The distal fragment is then flexed, internally rotated and translated anteriorly on the proximal fragment before fixation with a blade plate.
In severe SCFE, PFO on its own may not be sufficient to restore a more normal head–neck offset, and the metaphyseal bump may still cause FAI [63, 64]. Whiteside and Schoenecker [63] have demonstrated that combining valgus derotational osteotomy with cervical osteochondroplasty leads to more desirable outcomes in terms of ROM and providing a satisfactory weight-bearing surface.
In order to prevent the occurrence of this deformity and the ensuing FAI, as well as acute, unstable SCFE, a modified version of Dunn's procedure may be used to manage unstable SCFE [65, 66]. The modification was made to Dunn's procedure by employing the dislocation technique described by Ganz et al. [45] to allow an extended retinacular soft tissue flap. Ziebarth et al. [66] reported no incidence of osteonecrosis, whereas Slongo et al. [65] noted one case in 23 patients. All authors concluded that the modified Dunn's procedure resulted in low complication rates and allowed the restoration of more normal proximal femoral anatomy by full correction of the slip angle.
Arthroscopic assisted mini-open osteochondroplasty has a role in the treatment of FAI secondary to SCFE [2]. Leunig et al. [67] reported three cases of mild SCFE (slip angle between 15° and 30°) in paediatric/adolescent patients aged between 11 and 15 years treated with arthroscopic osteoplasty following in-situ pinning. This study reported a good outcome in all three patients in terms of symptoms and ROM, with no complications at follow-up, which ranged from 6 to 23 months. The authors concluded that this method is effective in limiting impingement after mild SCFE and recommended that in-situ pinning and arthroscopic osteochondroplasty could be performed concomitantly or in a staged fashion.
LCPD
The surgical management of adolescents with FAI secondary to LCPD is aimed at improving the ROM by reducing impingement, restoring joint congruency and maintaining/improving stability. It is vital to establish whether FAI is intra- or extra-articular, and femoral or acetabular, pre-operatively in order to plan surgical treatment effectively.
Various surgical procedures to correct the deformity on the femoral side have been described: inter-trochanteric osteotomy [68], relative neck lengthening with trochanteric distalisation [69] and femoral head reduction osteotomy [70]. Ganz et al. [70] have shown that their surgical approach for hip dislocation and osteochondroplasty can be applied to hips affected by LCPD, allowing full inspection and dynamic assessment of the femoroacetabular contact during hip motion.
Anderson et al. [71] treated 14 patients with LCPD using SDO with trochanteric advancement. Intra-operative findings included four femoral osteochondritis dissecans (OCD), which were treated with autografts created from the femoral osteochondroplasty resection. The average HHS improved from 63 pre-operatively to 95 post-operatively in the presence of an OCD lesion, and from 71 to 88.6 in the absence of OCD lesions. The authors pointed out the high rate of femoral head OCD lesion in LCPD and concluded that SDO and trochanteric advancement reduces the impingement, improves hip joint biomechanics and allows the treatment of intra-articular pathology.
PAO has been used to treat acetabular dysplasia with instability secondary to an aspherical femoral head [72]. Siebenrock et al. [73] reported the outcome of PAO in the treatment of anterior FAI in 29 hips in mixed adolescent and adult patients. The average Merle d'Aubigné score increased from 14.0 points pre-operatively to 16.9 points post-operatively (p < 0.001), and the result was good or excellent for 26 hips.
Due to the complexity of the deformity that could occur in LCPD, it can be challenging to differentiate the patients with isolated FAI from patients with hip instability caused by secondary acetabular dysplasia or a combination of both [34]. For this reason, a combined approach may be needed [72, 74]. Clohisy et al. [72] treated 26 hips with acetabular dysplasia secondary to proximal femoral deformity using the Bernese PAO, 13 of which were combined with proximal femoral valgus osteotomy. The mean HHS increased from 68.8 pre-operatively to 91.3 at final follow-up (p < 0.0001).
An algorithm for the surgical management of acetabular retroversion has been recommended by Peters et al. [75]. This algorithm takes into account the degree of acetabular coverage (lateral centre edge angle and the posterior wall sign) and the condition of the acetabular cartilage. The algorithm directs surgical treatment towards acetabular rim debridement, provided that the lateral centre edge angle (CEA) is less than 20° and there is no crossover sign irrespective of the acetabular cartilage condition. If the CEA is greater than 20° and the crossover sign is present, the choice of intervention depends on the condition of the acetabular cartilage. PAO is recommended only if the acetabular cartilage is intact. If damaged, surgical dislocation with rim debridement with or without femoral osteochondroplasty is recommended, as acetabular reorientation in this scenario would position the damaged cartilage in the main weight-bearing area [54]. Using this algorithm, the HHS improved from 52 to 90 in the hips treated with surgical dislocation and osteochondroplasty and from 72 to 91 in the hips treated with PAO.
Operative technique of SDO
This technique was originally described by Ganz et al. [45]. We have described the steps below, including the original technique along with some of our personal preferences.
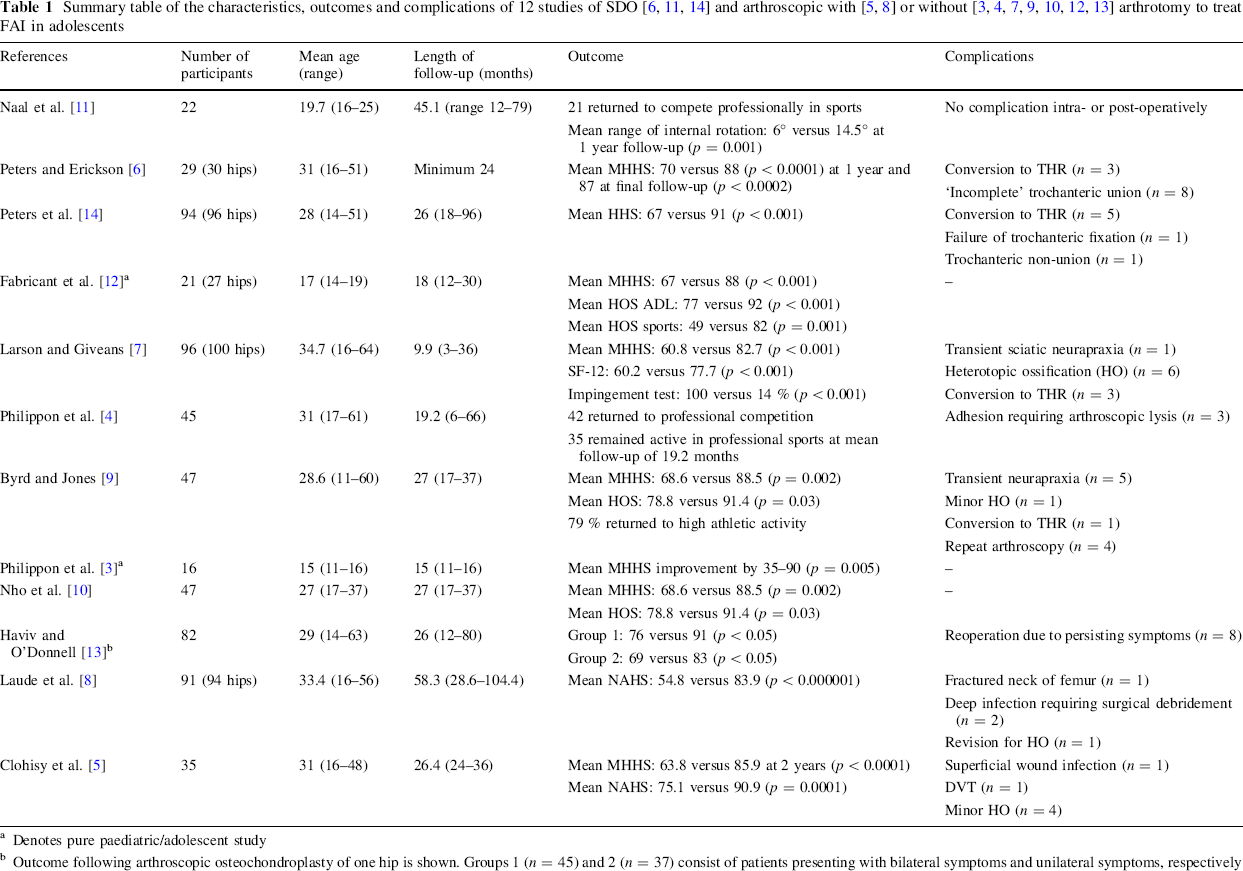
The patient is placed in a lateral decubitus position using a Stulberg lateral positioner on a radiolucent table. A modified Gibson incision is used to expose and divide the interval between the tensor fascia and gluteus maximus. The latter is retracted posteriorly to expose the posterior border of gluteus medius. An extra-articular trochanteric flip osteotomy is performed, running from the lateral margin of the piriformis fossa to the vastus lateralis ridge. The blood supply to the femoral head is mainly from the deep branch of the medial femoral circumflex artery [76, 77] and is protected by preserving the short external rotators of the hip. The osteotomised fragment should have a small sleeve of the gluteus medius and vastus lateralis attached, and is retracted anteriorly to expose the capsule. A Z-shaped capsulotomy is made to expose the hip joint and the femoral head can be dislocated anterosuperiorly (Fig. 2).
Intra-operative photographs of
Femoral osteochondroplasty is performed with or without the use of intra-operative templates to remove the cam lesion to restore the femoral neck clearance and permit impingement-free ROM of the hip. Sufficient bone should be removed to allow 120° of flexion and 40° of rotation [16].
The need for intervention on the acetabular rim is dependent on whether there is anterior over coverage and the extent of labral and articular cartilage damage [44]. We use a morphologic system to document the severity and location of labral and cartilage damage in all cases. If anterior overcoverage is present, osteoplasty can be performed from the anterosuperior rim using an osteotome or a high-speed burr after carefully detaching the labrum. Up to 1.0 cm of acetabular rim can be removed without causing joint instability [16]. The labrum has an important role in the normal hip function; therefore, it should be preserved as much as possible and only be excised if it is ossified, extensively scarred, or degenerated [44]. The labrum should be reattached using non-absorbable/partially absorbable anchor sutures. The capsular edges should be loosely approximated with absorbable sutures, as overtightening may compromise the retinacular perfusion due to kinking of the vessels [78]. The trochanteric osteotomy is fixed using two (our preference) or three cortical screws centred in the osteotomy fragment and aimed towards the lesser trochanter [16].
The advantage of this technique is that it allows intra-operative ROM assessment and 360° assessment of the proximal femur and the acetabulum under direct vision [45]. Procedures such as relative femoral neck lengthening and femoral neck osteotomy can be performed in combination if osteochondroplasty alone is not adequate to prevent impingement [6, 45, 71].
Post-operatively, most studies advocate a period of 6–8 weeks of toe-touch weight-bearing [6, 11, 44, 45]. Our personal protocol is toe-touch weight-bearing for 6 weeks, followed by gradual increase in weight-bearing to full weight-bearing over a 2-week period, with hip strengthening exercises starting at 6 weeks. Flexion is limited to 70° and NSAIDs may be used for the first 2 weeks for heterotopic ossification prophylaxis [11, 43].
Ganz et al. [45] reported two cases of sciatic neurapraxia, three trochanteric non-unions and 11 cases of heterotopic ossification of clinical significance. In a mixed series of young adults and older patients, Sink et al. [79] have recently reported on a multi-centre study regarding complications after surgical dislocation. This study included 334 hips in 302 patients, with mean age of 26 years (range 8–61 years). The patients were followed up for an average of 5.8 months (range 2–11 months). The overall incidence of complication was 9 %. They reported no cases of osteonecrosis, femoral neck fracture or any complication leading to long-term morbidity. There was one sciatic nerve injury, which partially resolved.
Operative technique of arthroscopic treatment
Hip arthroscopy is commonly performed under general anaesthesia, with the patient positioned supine or in the lateral decubitus position [80, 81]. The choice of position simply depends on the preference of the operating surgeon, but the lateral approach may be preferable in severely obese patients [81].
The hip joint has a central compartment (where the labrum, femoral head and acetabular cartilage, amongst other structures, can be visualised) and a peripheral compartment (where the femoral head–neck junction is seen) [82, 83]. A standard fracture table and a heavily padded perineal post are needed in order to achieve effective joint space distraction. The perineal post should be lateralised against the medial thigh to achieve the optimal traction vector and to reduce direct pressure on the perineum and pudendal nerve.
Standard portals include anterolateral, posterolateral and anterior. Both anterolateral and posterolateral portals are placed along the superior margin of the greater trochanter at the anterior and posterior borders, respectively. The anterior portal is sited where a sagittal line extending distally from the anterior superior iliac spine intersects a transverse line across the tip of the greater trochanter [84]. We prefer to use a distal mid-anterior portal as our second portal following the anterolateral portal, which is sited midway between the anterior and anterolateral in order to avoid branches of the lateral femoral cutaneous nerve.
Using an image intensifier, a spinal needle is inserted into the hip joint anterolaterally to distend the joint with fluid before a trochar is introduced. A 70° scope is used to guide the placement of further portals under the direct arthroscopic view. The procedure usually begins with inspection of the central compartment. Pincer lesions are typically identified in the superior acetabular quadrant [4], which can be trimmed if moderate or large using a motorised burr [85]. Small pincer lesions (2–3 mm) may not require trimming, as the treatment of the cam lesion may relieve the impingement [86]. Damaged labrum may be debrided until stable or repaired, depending on the nature of the damage. Detached and peripheral mid-substance tears can be repaired using suture anchors [85, 87]. The condition of the acetabular cartilage should be assessed and can be graded using various classification systems, including the Outerbridge system [88]. If sub-chondral bone is exposed, micro-fracture may be performed [89].
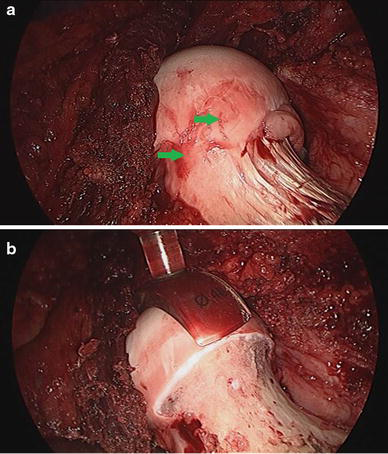
The traction should be released once central compartment assessment is completed. The arthroscope is introduced into the peripheral compartment using the anterolateral portal to evaluate the femoral head–neck junction (Fig. 3). Cam lesions should be resected under fluoroscopy using a motorised burr, taking care to avoid the lateral epiphyseal vessels [4].
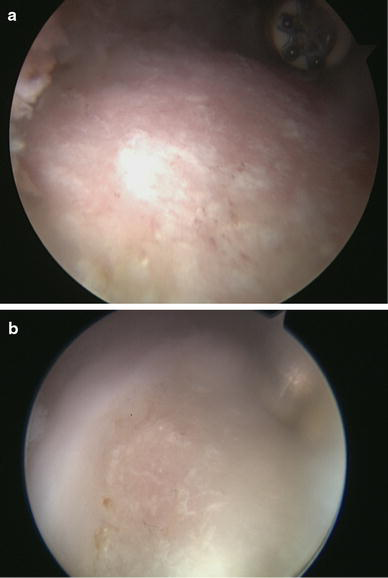
Intra-operative images of hip arthroscopy during assessment of the femoral head–neck junction in the peripheral compartment
There are various factors that can make hip arthroscopy technically challenging in the adolescent population, such as the presence of open physes, smaller volume hip joints and deformity secondary to previous hip disease, such as LCPD [2]. In LCPD, access to the peripheral and central compartments may be difficult, due to proximal femoral deformities such as coxa magna and brevis.
Complications associated with the arthroscopic treatment of FAI include deep vein thrombosis, neurapraxias, particularly of the lateral femoral cutaneous nerve, femoral neck fractures, avascular necrosis, iatrogenic chondral damage, myositis ossificans and heterotopic ossification [90]. Two studies have reported complications in paediatric and adolescent patients following hip arthroscopy: transient pudendal nerve palsy (n = 5), instrument breakage (n = 2), suture abscess (n = 1) and recurrent labral tears (n = 3) [91, 92].
Hip arthrodesis and arthroplasty
Despite the positive early clinical results of the various joint-preserving surgeries discussed, a small number of adolescents, who have severe hip degeneration at the time of presentation, tend to have poor outcomes following such procedures [93]. These patients may require joint arthroplasty in the short to medium term [93, 94]. Hip arthrodesis is less commonly used today due to advances in arthroplasty technique, but may be considered in selected young adults [56].
Studies of total hip arthroplasty in adolescents have small sample sizes and short-term follow-up, making it difficult to generalise their results. Kamath et al. [95] reported their outcome of modern-alternative total hip arthroplasty in patients with a mean age of 18 years (range 13–20 years). Significant improvement in HHS (43.6 vs. 83.6, p < 0.001) at an average follow-up of 49 months (range 25–89 months) and no radiological evidence of loosening was noted at final follow-up.
Earlier studies report loosening rates or radiological evidence of failure as high as 57 % at less than 11 years follow-up [96, 97]. More recently, Busch et al. [98], in a retrospective study to evaluate the survival rate of cemented components with bone impaction grafting in patients under 30 years old (range 16–29 years), found a 10-year survivorship of 83 %, with revision as the endpoint. This survival rate is comparable to the rates found in total hip arthroplasty in elderly adults [99].
Total hip arthroplasty in adolescents can be technically challenging due to previous surgery and/or underlying deformity, and many of these patients will require revision during their lifetime [100]. These are the important factors that must be taken into account during pre-operative planning in order to optimise outcomes of hip reconstruction in this group of patients. It is likely that the long-term outcomes of total hip arthroplasty in this group of patients will improve with time.
Summary
FAI is being increasingly recognised in adolescents and paediatric patients. There are various treatment options available to address symptomatic FAI, and the choice of surgery should be tailored to the individual patient's hip morphology and severity of involvement, as well as recovery expectations.
Arthroscopic treatment of FAI allows faster post-operative recovery when compared to those treated with open surgical dislocation, and the initial results are favourable and comparable to open surgery. There is certainly a spectrum of cases that need open procedures and more extensive surgery. Early correction of symptomatic FAI may reliably improve hip pain, but long-term studies are required in order to determine whether such interventions predictably prevent the progression of symptomatic FAI to OA of the hip.