
Abstract
Abstract
Background
Pediatric supracondylar humerus fractures commonly require surgical intervention and hospital admission, which is costly and consumes significant health care resources. There are few data regarding temporal characteristics (month, day and hour of injury) of this particular pediatric fracture. We wished to investigate the month, day of the week, and time of occurrence of these fractures to guide appropriate use of health care resources and prevention strategies.
Methods
This study was a retrospective review of clinical records and radiographs of 353 children with operative supracondylar humerus fractures in a temperate climate region over 6 years. Date and time of injury and demographic data (gender, age, laterality) were extracted. Variation in month, weekday, and time of injury was analyzed using circular analysis, cosinor analysis, probability distributions and topographical distribution.
Results
There was a statistically significant increase in the number of fractures during the summer with a peak in early July. When analyzing by month and day of the week, a peak was seen Thursday-Saturday during May–July and middle of the week September–October. Weekdays demonstrated a higher proportion of fractures occurring in the morning and at school. The injuries occurred in the am in 37 and the pm in 241; detailed data were known in 227 with 37 between 0000 and 1159, 51 between 1200 and 1559, and 139 between 1600 and 2359 h. The peak time of injury was 1800 h.
Conclusions
The increase in supracondylar humerus fractures in the spring through autumn in temperate regions indicates that education campaigns reinforcing fall prevention and landing surfaces should be done in the early spring. The hourly data support the need for dedicated early morning operating rooms to care for these fractures.
Level of evidence
Prevalence study, retrospective cohort, Level II.
Introduction
Displaced pediatric supracondylar humerus fractures require surgical intervention and hospital admission, which is costly and consumes significant health care resources. Numerous studies review the treatment and outcomes of this fracture; most demographic data focus on age, gender, and laterality. There are few data regarding temporal characteristics (month, day, and hour of injury). A few authors [1–6] have discussed such data but none have subjected their data to rigorous statistical and/or mathematical analysis. The purpose of this study was to analyze the month, day of the week, and time of occurrence of operative supracondylar humerus fractures treated at the authors’ institution. Significant patterns can be used to guide appropriate use of health care resources and prevention strategies.
Materials and methods
A retrospective review was performed of all children admitted to the authors’ institution with supracondylar humerus fractures undergoing operative stabilization from 2004 to 2009. This institution was in a temperate region having all four seasons. All fractures were type II and III severity using the Gartland classification [7] (type I—non-displaced; type II—posterior hinge intact but with anterior apex angulation; type III—completely displaced). Type I fractures do not need surgery and thus were excluded. Radiographs were reviewed to confirm the diagnosis and fracture type. Date and time of injury, as well as standard demographic data (gender, age, laterality) were obtained from the medical record. The study was approved by our Institutional Review Board.
Statistical analysis
Discrete data are reported as frequencies and percentages and continuous data as the mean ± 1 standard deviation. Differences between groups of discrete data were analyzed by the Pearson's χ2 test (Systat 10 software™, Chicago, IL, 2000).
Variation in month, weekday, and time of injury was first examined with circular analysis [8]; the Rayleigh z-test was used to test the null hypothesis that the temporal distribution was uniform. Statistically significant differences were further analyzed with cosinor analysis, which represents the mathematical best fit of the data to a cosine curve defined by the equation

where M = the mean level (termed mesor), A = the amplitude of the cosine curve, ϕ = phase angle of the maximum value (also termed acrophase), ω = the frequency (which for monthly analysis is 360°/12 = 30°, for weekday analysis is 360°/7 = 51.4°, and for time of day is 360°/24 = 15°), and t = time. If the overall p value for the goodness of fit of this equation reaches statistical significance, then the data are not a uniform circular distribution, but rather represent a rhythmic pattern described by the cosinor equation using M, A, and ϕ. Cosinor analyses were performed with ChronoLab 3.0™ software. Cosinor analysis can only be used on symmetric data having a zenith and nadir. Skewed data were analyzed with probability distributions (EasyFit Professional™ 5.0 software, © Math Wave Technologies, Plimus, 2008). For all analyses a p < 0.05 was considered statistically significant.
Distributions by weekday and month were analyzed using a method analogous to a topographical map using “contours of elevation” [9]. The number of fractures was plotted onto a topographic “map” with the month on the x axis, the weekday on the y axis, and the number of fractures on the z axis (or “elevation” of the contour) (DPlot™ software, version 2.2.4.6, HydeSoft Computing, Vicksburg, MS, 2008).
Results
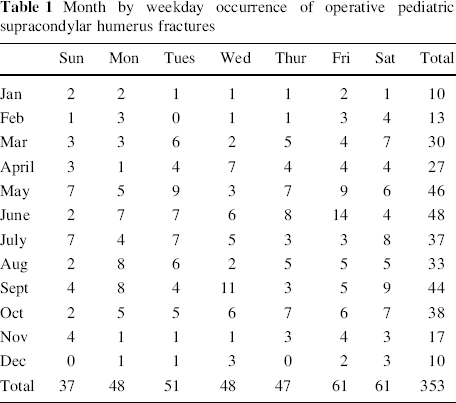
There were 353 children (178 boys, 175 girls) (Table 1) with supracondylar humerus fractures that underwent surgical intervention. The average age was 5.9 ± 2.7 years. The injury (when known) occurred on playground equipment in 101, furniture in 68, other climbing activities in 56, sports in 36, trampolines in 34, bicycles in 17, and all terrain vehicles (ATVs) in 16. There were 147 right and 187 left sided fractures (unknown in 9). The location of injury (when known) was the home in 160, public property and sporting locations in 74, and schools in 35. The injuries occurred in the am in 37 and the pm in 241; more detailed data were known in 227 with 37 between 0000 and 1159, 51 between 1200 and 1559, and 139 between 1600 and 2359.
Month by weekday occurrence of operative pediatric supracondylar humerus fractures
Temporal analyses
There was a statistically significant increase in the number of fractures during the summer with a peak in early July (Fig. 1). Summer peaks were noted for both boys (July 21) and girls (July 13). When analyzing by subsets, the peak time when injured on playgrounds was June 29, trampolines June 23, bicycles May 5 and ATVs June 7; no peaks were noted for climbing activities, furniture, or sports activities. No statistically significant differences were noted by day of the week or by subsets of injury mechanism or gender. When analyzing by both month and day of the week, a peak was seen in aggregate for Thursday-Saturday during May–July and middle of the week September–October (Fig. 2).
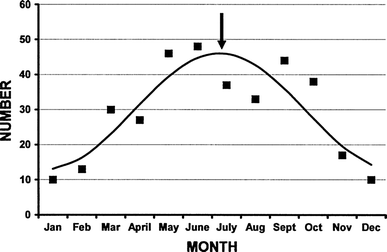
Occurrence of pediatric supracondylar humerus fractures by month. This distribution was statistically significant (Rayleigh z = 27.95, p < 0.001), with a peak occurrence on July 10 (arrow). Using cosinor analysis, the data can be fit to a curve represented by the equation: number of fractures = 29.5 + 16.5 cos (30t − 188), where t = the time in months (1 = January, 2 = February, etc.) (r2 = 0.76, p = 0.002)
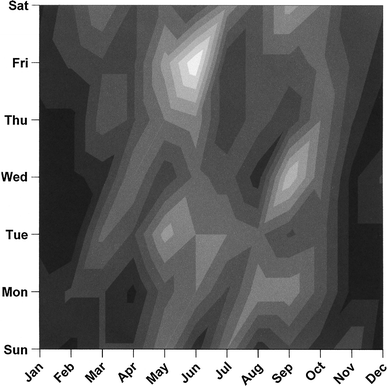
Topographic contour representations of operative supracondylar humerus fractures in a weekday by month visualization. The month is on the x axis and the weekday on the y axis. The lowest contour (fewest fractures) is black and the highest contour (most fractures) is white. Note the peaks in May–July Thursday–Saturday, and September Tuesday–Thursday
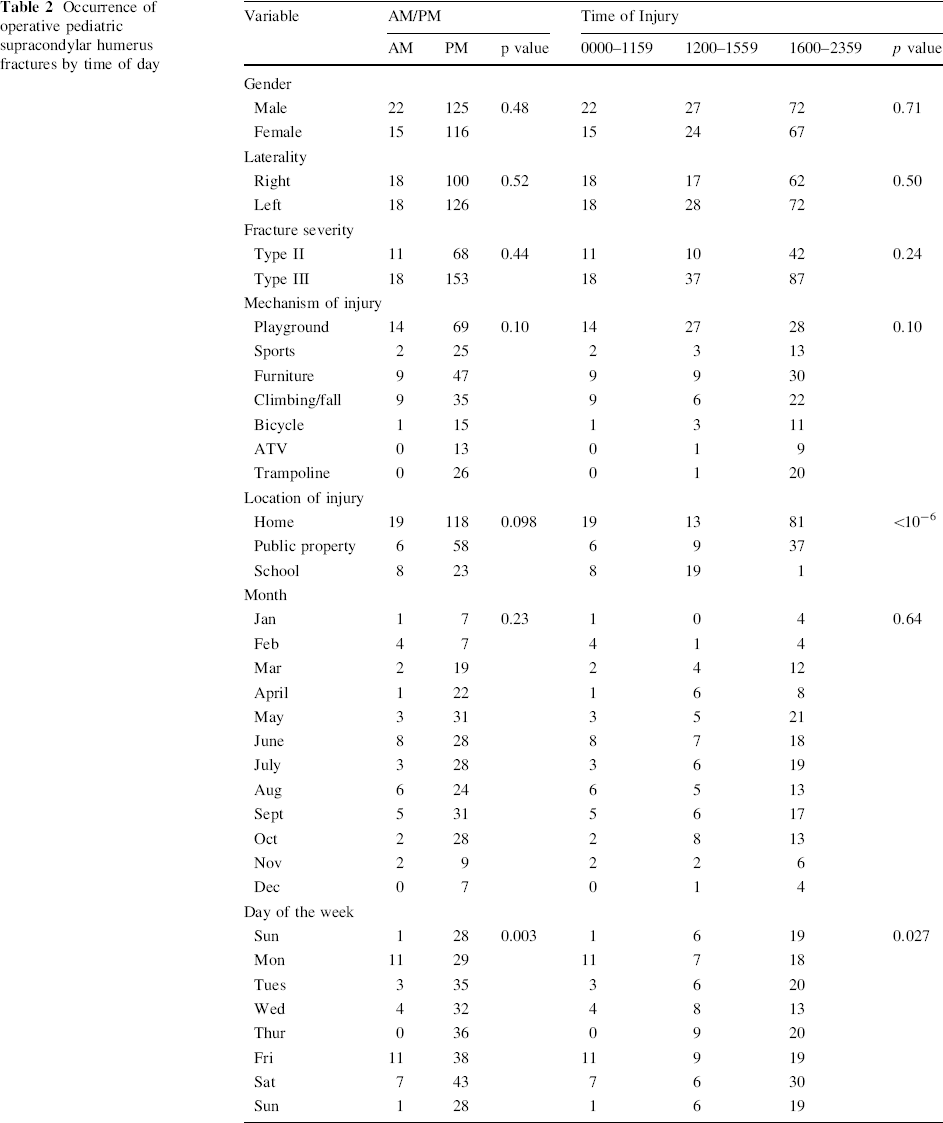
In 278 cases, the data were adequate to determine if the fracture occurred in the am or pm (Table 2). There were statistically significant differences by am/pm time only in the day of the week. When dividing the time of the day into three groups (0000–1159, 1200–1559, and 1600–2359), differences were noted for day of the week as well as location of where the injury occurred by time of day. This particular time of the day was chosen to represent three major groups—midnight through noon, afternoon, and evening/night. Weekdays demonstrated a higher proportion of fractures happening in the morning and at schools. The time of injury within 1 h segments was known for 181 children (Fig. 3). For this skewed data a peak occurred at 1800 h (Johnson S B distribution [10]).
Occurrence of operative pediatric supracondylar humerus fractures by time of day
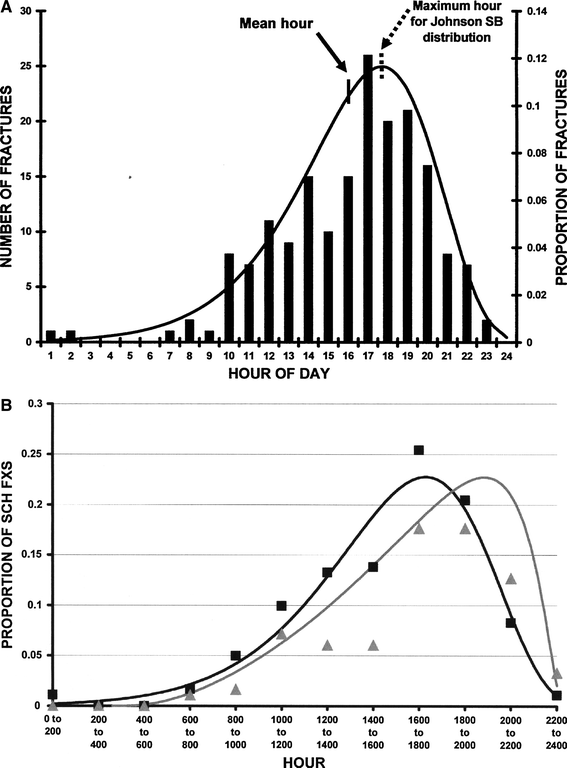
Time of injury for supracondylar humerus fractures.
Discussion
Few studies investigate temporal variation in pediatric fractures. In Malmö, Sweden, 589 elbow fractures were studied; 320 (55 %) were supracondylar humerus fractures [4]. The peak months of injury were July–September. Another study of 355 pediatric elbow fractures in Esjberg, Denmark [6], where 204 (57.5 %) were supracondylar humerus fractures, also found a summer peak. In a review of 6,493 fractures in Hong Kong children <16 years of age [3] a peak incidence was noted in late September and October, coinciding with the start of school and the finest local weather. In San Diego, California the seasonal trend was less pronounced (37 % June–September and 29 % November-February) [1] due to similar year round weather.
In this study originating from a temperate climate region, a July 10 peak was noted using cosinor analysis. Other studies demonstrate similar summer peaks: July 2 for Ejsberg, Denmark [6] and Hong Kong (children 8–11 years only) [3], and July 30 in Malmö, Sweden [4] (Fig. 4). Monthly variations can be used for prevention programs. Recent research has been performed regarding appropriate playground landing surfaces [11–18] and maximum heights [12, 14, 17, 19], resulting in efforts to improve landing surfaces of playground equipment. Several studies noted significant reductions in equipment related hazards [20, 21] as well as injury rates [22] when less than optimal equipment and/or landing surfaces are corrected. Knowing that there is a peak in supracondylar humerus fractures in the spring and fall, the best times to check on the status of landing surfaces is before these peaks [23]. Education campaigns reinforcing the need to check these surfaces should be done in the early spring and late summer.
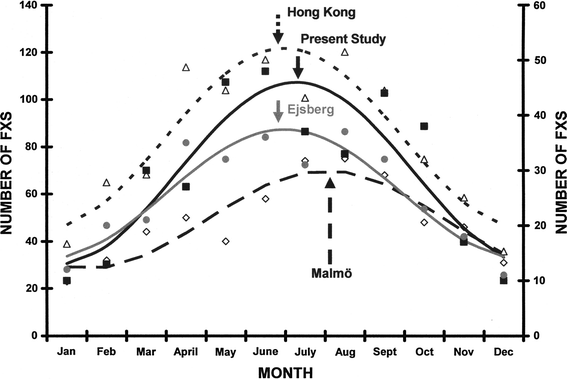
Peak occurrence of pediatric fractures using cosinor analysis. The data come from the present study of supracondylar humerus fractures (solid squares, solid black line best fit; July 10 peak, solid black arrow) as well as pediatric elbow fractures in Malmö, Sweden [4] (open rhomboids, long hatched black line best fit; July 30 peak, long hatched black arrow), pediatric elbow fractures in Ejsberg, Denmark [6] (gray circles, gray line best fit; July 2 peak, gray arrow) and Hong Kong children age 8–11 years encompassing all fractures (open triangles, short hatched black line best fit; July 2 peak, short hatched arrow). These were all significant (p < 0.002, r2 ≥ 0.76). The number for the studies from Hong Kong and Malmö are shown on the left y axis and for Ejsberg and the present study on the right y axis
A previous study investigated the injury day of the week for supracondylar humerus fractures and no differences were noted [1]. This was confirmed in aggregate in this study, but when analyzing day of the week by month, peaks were noted in Thursday-Saturday during May–July and a lesser peak in the middle of the week in September–October (Fig. 2). We also noted that during the weekdays, more morning fractures occurred than on weekends. These usually occurred at school, and likely due to morning school recess times during school days.
Few studies mention the hour of injury in pediatric fractures. Mangwani [24] reviewed 291 pediatric supracondylar humerus fractures in London, England, and reported the time of presentation to the hospital but not the hour of injury. In Khartoum, Sudan, 231 pediatric fractures of all types [5] were studied; most occurred between late afternoon and sunset. In Kuala Lumpur, Malaysia [2], 64 of 132 supracondylar humerus fractures (48.9 %) occurred between 4 and 8 pm. In this study 44.4 % (79 of 181) occurred between 4 and 8 pm, with a peak at 1800 (Fig. 3a). When comparing the data between Kuala Lumpur and the present (Fig. 3b), the peak hour of injury was 1800 in the present study and 2000 in Kuala Lumpur. This may be due to a more tropical climate in Kuala Lumpur, equal hours of sunlight throughout the year in an equatorial location compared to the temperate climate in this study, or cultural differences regarding time of school dismissal and supper.
A potential criticism of this study is the accuracy of the time of injury—did the parents accurately remember the time which was recorded in the hospital record? It has been shown that parents accurately recall the time of injury during a stressful event [25] if accuracy less than 10 min is not needed. In this study, we used differences of an hour, not 10 min, so our 1 h incremental data is likely very accurate. It is also possible that the time of injury for all 353 cases might be different than the 181 recorded cases. We compared the 181 children whose time was recorded to the 172 where it was not; there were no statistically significant differences by age gender, laterality, or fracture severity between these two groups. These 181 cases thus likely represent all 353 cases. This is reinforced by the similarities between our data and that in Malaysia confirming the accuracy of our data [2]. The peak occurrence in the late afternoon and early evening peak translate to a significant proportion of these children being admitted at the definitive treatment facility late in the day [1] after being evaluated at several other medical care facilities [26, 27], arriving at the definitive tertiary care children's hospitals late in the night or early am. This supports the need for dedicated night and early morning operating rooms to care for these fractures, allowing for timely care with knowledgeable surgical teams without impacting the regular OR day [27]. Although some institutions have such dedicated OR time, not all do. This study further reinforces the need for such capabilities, which should result in fewer complications [28, 29], shorter OR times [28], and overall improved OR efficiency [27, 28].
Conclusion
Operative supracondylar humerus fractures are a common childhood injury that consume significant health care resources. Knowing that the majority of these injuries occur late in the day demonstrates the need for dedicated night and early morning surgical suites to care for these fractures. The increase in the spring through fall in temperate regions indicates that education campaigns reinforcing fall prevention and landing surfaces should be done in the early spring.
Footnotes
None.
Acknowledgments
ChronoLab 3.0™ software, designed for use on Macintosh™ computers, cannot be purchased. The software used to perform cosinor analyses was provided through the courtesy of Dr. Atremio Mojón and colleagues, Bioengineering and Chronobiology Labs, ETSI Telecomunicación, University of Vigo, Campus Universitario, Vigo (Pontevedra) 36280, Spain. It can be downloaded from their web site at ![]() . Please kindly acknowledge their generosity when using this software. This research was supported in part by the Garceau Professorship Endowment, Indiana University, Department of Orthopaedic Surgery, and the Rapp Pediatric Orthopaedic Research Endowment, Riley Children's Foundation, Indianapolis, Indiana.
. Please kindly acknowledge their generosity when using this software. This research was supported in part by the Garceau Professorship Endowment, Indiana University, Department of Orthopaedic Surgery, and the Rapp Pediatric Orthopaedic Research Endowment, Riley Children's Foundation, Indianapolis, Indiana.
Addendum
The bounded Johnson S B distribution is represented by the equation
where f(x) = the proportion at any time x, ξ is the location parameter, λ the range parameter, and λ and γ are shape parameters. For the best fit of these 181 cases, the values for these parameters were γ = −8.3182, δ = 3.0653, λ = 18,762.0, ξ = −15,926.0 (EasyFit Professional™ 5.0 software, © Math Wave Technologies, Plimus, 2008).