
Abstract
Abstract
Purpose
Pediatric tibial shaft fractures are common injuries encountered by the orthopaedic surgeon. Flexible intramedullary nailing has become popular for pediatric patients with tibial shaft fractures that require operative fixation. The purpose of our study was to evaluate the incidence of, and the risk factors for, compartment syndrome (CS) after flexible intramedullary nailing of these injuries.
Methods
A retrospective review of tibial shaft fractures treated consecutively with flexible intramedullary nailing at our institution from 2003 to 2010 was performed. The incidence of CS after flexible nailing was recorded. In addition, age, weight, mechanism of injury, polytrauma, presence of an open fracture, presenting neurovascular exam, fracture pattern, delay in treatment (>24 h from injury), prior closed reduction attempts, method of reduction (open vs. closed) in the operating room, total fluoroscopy time, and operative time were recorded. Comparisons were made between children who developed CS and those who did not.
Results
Thirty-one children met inclusion criteria with a mean age of 11.2 years (range, 6.3–15.3 years); all were boys. Nearly, 20% of children developed CS after flexible nailing of their fractures. Those who developed CS after flexible nailing were heavier than the unaffected group (52.6 ± 14.5 kg vs. 39.4 ± 15.2 kg, P = 0.05); with a greater percentage of children 50 kg or greater (83.3% vs. 26.1%, P = 0.02) within the CS group. Children who developed CS were also more likely to present with neurologic deficits in the absence of compartmental swelling prior to surgery (66.7% vs. 9.1%, P = 0.009), and more likely to have comminuted/complex fracture patterns (83.3% vs. 29.1%, P = 0.02). There was no difference between patients who did and did not develop CS in regards to age (P = 0.42), high-energy injury mechanism (P = 0.30), polytrauma (P = 1.0), delay in treatment (P = 0.28), prior closed reduction attempts (P = 1.0), method of reduction (open vs. closed; P = 1.0) in the operating room, total fluoroscopy time (P = 0.96), and total operative time (P = 0.45). In addition, there was no difference (P = 0.65) in the rates of CS between children with open and closed fractures.
Conclusions
There is a high risk of CS after flexible intramedullary nailing of pediatric tibial shaft fractures regardless of whether an injury is open or closed. Variables that would seemingly be associated with the development of CS (high-energy injury mechanisms, polytrauma, treatment delay, prior closed reduction attempts, and closed reduction in the operating room) were not statistically associated with CS in our study. Clinicians should be wary for the development of CS whenever utilizing flexible nails for tibial shaft fractures, especially when the following co-morbidities are present: the child weighs greater than 50 kg, has complex/comminuted fracture patterns, or has a neurologic deficit in the absence of compartmental swelling prior to operative intervention.
Introduction
Fractures of the tibia and/or fibula are the second most common fracture leading to pediatric orthopaedic admission [1, 2], and a variety of methods exist to treat these injuries including closed reduction/casting [3], external fixation [4–6], and plating [7]. Recently, flexible intramedullary nailing has become the preferred method for the treatment of tibial shaft fractures that require operative fixation [6, 8–13].
Developed in the Nancy region of France, flexible intramedullary nailing is predicated on the use of two pre-bent elastic nails crossing each other at the level of the fracture within the medullary canal placed in an un-reamed fashion [14]. Efficacy of this technique is augmented when utilizing implants that encompass 80% of the diameter of the medullary canal at its narrowest point [12]. The advantages of this technique include stability, flexible mobility, and the ability to perform a closed reduction with minimal disruption of the soft tissue and periosteal blood supply. Yet, complications have been reported with the use of flexible nailing, particularly, in older, heavier patients with unstable/complex fracture patterns [10, 15, 16].
In addition, tibial shaft fractures have been shown to be at high risk for the development of compartment syndrome (CS) in the pediatric population, presenting as the most frequent fracture linked with this condition [17–20]. Studies looking specifically at flexible nailing of tibia fractures have cited rates of CS as high as 32.0%, yet it is unclear from these studies if CS occurred before or after flexible nailing had been performed [8, 11, 21, 22]. Although the risk of CS after flexible nailing of forearm fractures has been noted to be as high as 10.0% [23], there has not been a specific study in the literature examining the risk for CS after flexible nailing of tibia fractures.
The purpose of our study was to evaluate the incidence of, and the risk factors for CS after flexible intramedullary nailing of pediatric tibial shaft fractures. We hypothesized that there would be identifiable risk factors that predict the development of CS after flexible nailing of these injuries in the pediatric population.
Materials and methods
This was a retrospective review examining tibial shaft fractures consecutively treated with flexible nailing from 2003 to 2010. Children with operatively treated tibia fractures were identified via a computerized search of our institution's billing database utilizing the CPT code 27759 (treatment of tibial shaft fracture with or without fibular fracture with intramedullary implant). Children were included in the study if they sustained a tibial shaft fracture with open proximal tibial physes, which was treated in the operating room with flexible nailing as their definitive treatments. Exclusion criteria included: treatment with modalities other than flexible nails for their tibia fractures (casting, external fixation, rigid nailing, plating, Kirschner wires), documented CS and/or fasciotomies performed prior to flexible nailing, surgery at an outside institution presenting to us for post-operative management, had flexible nails placed for delayed unions, non-unions, malunions, or had pathologic fractures, neuromuscular disorders, skeletal dysplasias, and/or metabolic diseases affecting the bone. The choice of flexible nailing for fracture treatment was based on surgeon preference.
Data collected from the chart review included: age at time of injury, gender, weight (kilograms), and mechanism of injury. Emergency room records were analyzed for the presence of pre-operative associated injuries (both orthopaedic and non-orthopaedic), neurovascular deficits, the presence of an open fracture, and reduction attempts in the emergency room. Radiographs were reviewed to determine whether fractures were transverse (simple) or comminuted (complex). Peri-operative data collected included: treatment delays (time to operating greater than 24 h after injury), procedures performed (including fasciotomies), implants utilized, method of reduction in the operating room (open vs. closed), total fluoroscopy time, and total operative time. For patients who had multiple operations during the same time in which their tibia fracture was stabilized, we excluded data in regards to fluoroscopy and operative time if we were unable to ascertain what portion of the total fluoroscopy or operative time was spent solely on the tibia.
The incidence of CS was recorded as was the time at which CS was suspected, and the clinical exam findings at that time prior to pressure measurements. Pre-operatively, if patients presented with increased pressure/swelling in a compartment, paresthesias/anesthesia, paresis/paralysis, pain with passive stretch, intact pulses, and a “pink” extremity (the signs and symptoms of compartment syndrome; Fig. 1) [24], they were not taken to the operating room for flexible nailing and were therefore excluded from the study. If patients presented pre-operatively with only a few of the aforementioned signs (particularly paresis, pain with passive stretch, or paresthesias) in the absence of compartmental swelling, the signs and symptoms were attributed to the inciting trauma rather than compartment syndrome.
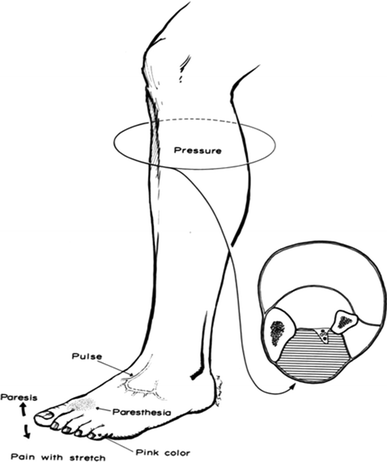
The six signs and symptoms of compartment syndrome. From [41]
For patients included in the study, the diagnosis of CS was made through measurement of compartment pressures at any time point after flexible nailing has been performed through the use of a slit catheter with an arterial line set-up [24]. Measurements were made in the anterior, lateral, superficial posterior, and deep posterior compartments. An absolute pressure measurement greater than 30 mm Hg was utilized to diagnose CS [24]. As all children were under anesthesia with artificially lowered blood pressure, differences between the measured compartment pressure and the diastolic blood pressure or mean arterial blood pressure were not utilized to diagnose CS [25].
Mean follow-up time was calculated from the date of surgery to final clinical follow-up. Residual neurologic deficits were noted at final follow-up. Means and standard deviations were calculated for all continuous variables. Children were divided into two groups based on the development of CS. Unpaired Student's t-test were used to determine whether significant differences existed between those with and without CS in regard to age, weight, total fluoroscopy time, and total operative time. Fisher's exact test was utilized to determine whether significant differences existed between those with and without CS in regards to mechanism of injury (high vs. low-energy), polytrauma, pre-operative neurovascular deficits, presence of open fracture, prior reduction attempts in the emergency room, fracture patterns (simple vs. complex), incidence of treatment delay (defined as time to operating room from injury >24 h), and method of reduction in the operating room (open vs. closed). Statistical significance was defined as P ≤ 0.05.
The Institutional Review Board for the University of California San Diego approved the protocol for this study before initiation.
Results
We identified 31 children with tibia fractures that underwent operative fixation with flexible intramedullary nails. They were all boys with open proximal tibial growth plates. The incidence of CS after flexible nailing was 19.3% (6 children; Fig. 2). Presenting neurovascular exam, clinical findings prior to pressure measurements, intra-operative pressure measurements after flexible nailing, intra-operative findings, number of flexible nails, methods of reduction in the operating room, wound management, and residual deficits are shown in Table 1 for patients who developed CS.
Development of compartment syndrome in patients treated with flexible nailing. CS compartment syndrome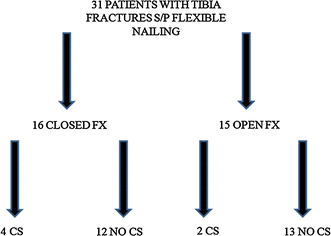
Pre-operative exam, time at which CS suspected, exam at time CS suspected, number of flexible nails, reduction utilized in the operating room, pressure measurements, surgical notes, and fasciotomy/residual deficit information for patients who developed CS
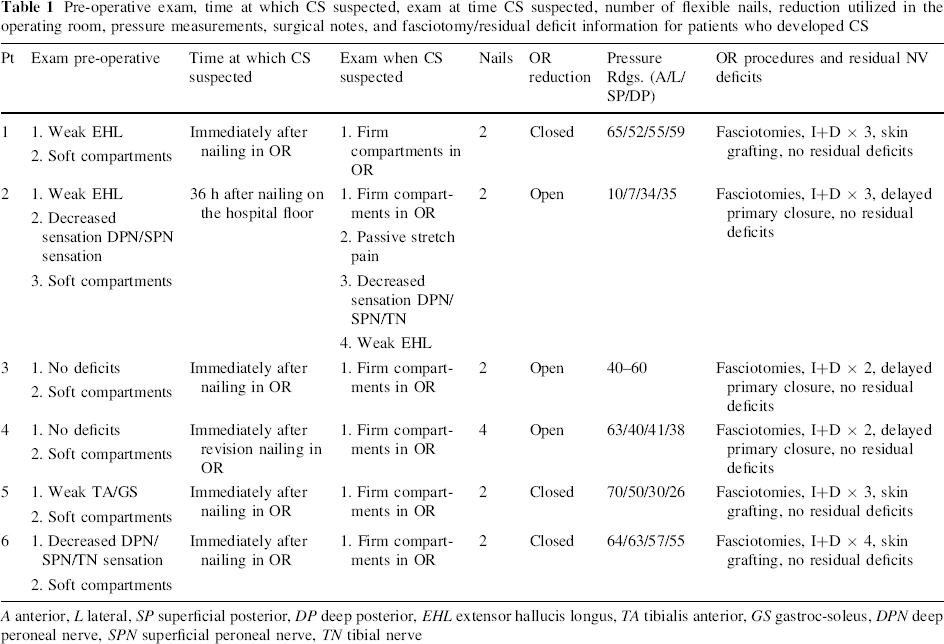
A anterior, L lateral, SP superficial posterior, DP deep posterior, EHL extensor hallucis longus, TA tibialis anterior, GS gastroc-soleus, DPN deep peroneal nerve, SPN superficial peroneal nerve, TN tibial nerve
The mean age of the boys with CS (12.0 ± 2.8 years) was not significantly different (P = 0.42) than those without CS (11.0 ± 2.6 years). Children with CS were heavier (52.6 ± 14.5 kg; P = 0.05) than the unaffected group (39.4 ± 15.2 kg); with a greater percentage (83.3% vs. 26.1%, P = 0.02) of those with CS weighing greater than 50 kg (Fig. 3). Children who developed CS were also more likely to present with neurologic deficits prior to surgery in the absence of compartmental swelling (66.7% vs. 9.1%, P = 0.009) and more likely to have comminuted/complex fracture patterns (83.3% vs. 29.1%, P = 0.02) (Fig. 4).
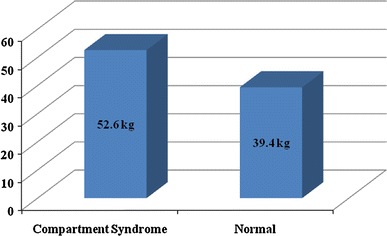
Mean weight of patients in CS versus non-CS group; P = 0.05
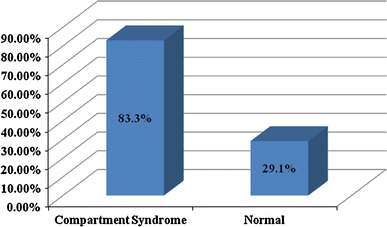
Percentage of patients with comminuted/complex fractures in CS versus non-CS group; P = 0.02
There was no difference between children who did and who did not develop CS in regards to high-energy injury mechanism (100.0% vs. 69.0%; P = 0.30), polytrauma (50.0% vs. 46.0%; P = 1.0), delay in treatment of injury greater than 24 h (0.00% vs. 33.3%; P = 0.28), prior reduction attempts in the emergency room (40.0% vs. 37.5%; P = 1.0), method of reduction (open reduction, 33.0% vs. 37.5%; P = 1.0) in the operating room, total fluoroscopy time (0.9 ± 0.6 min vs. 0.9 ± 0.7 min; P = 0.96), and total operative time (97.8 ± 39.6 min vs. 84.3 ± 32.5 min; P = 0.45). In addition, there was no difference (closed fracture 66.7% vs. 45.9%; P = 0.65) in the rates of CS between children with open and closed fractures. Total mean follow-up time was 12.3 ± 12.2 months, and no patients who developed compartment syndrome had residual neurologic deficits.
Discussion
With the residual effects originally described by Volkmann in 1881, CS is a condition in which elevated pressures within a fascial space caused by a variety of factors leads to decreased circulation, ischemia, and eventual tissue necrosis [26]. CS in adults has been studied extensively [25], although there has been limited literature in the pediatric population examining this condition [27–31]. The classic signs of CS in the adult population have been shown to be unreliable in children [31]. Bae et al. examined 36 cases of CS in children and found that increasing analgesia requirement was a more sensitive indicator for CS in children than those used in adults [31].
The etiology of CS can be varied in children although fractures, vascular injury, and tibial osteotomies are the most commonly cited [18, 30–33]. In 1979, Mubarak and Carroll reported that supracondylar humerus fractures treated with casts and femoral shaft fractures treated with traction were the most common injuries causing upper and lower extremity CS [27]. As fixation methods and reduction techniques have improved, the incidence of these specific injuries causing CS has decreased [31]. It is now clear that the leg is the most common location for CS in the pediatric patient. Grottkau et al. examined 139 cases of CS in children and adolescents over a 51-month period from the National Pediatric Trauma Registry [18]. The authors found that 90.0% of the lower extremity fractures causing CS were tibia-fibula fractures. Furthermore, Gal et al. found that 86.67% of their pediatric patients with CS had lower extremity involvement [19]. As a result, it is imperative for the clinician to recognize that fractures of the tibia present a high risk of CS; particularly as tibia fractures are the second most common reason for pediatric orthopaedic admission with an incidence of 110–190/per 10,000 [1, 2].
In regards to our nearly 20% incidence of CS, it is important to recognize that all of them occurred in children after flexible nailing of their tibia fractures. Therefore, it is important for clinicians to not only realize that tibia fractures (the injury) in the pediatric population are a general risk factor for compartment syndrome but also that flexible nailing (the treatment) poses a potential risk as well. In a similar study, Yuan et al. examined the incidence of CS in 285 pediatric forearm fractures [23]. The authors found a 10% rate of CS in children who underwent closed reduction and intra-medullary (IM) fixation, and a 6.0% rate in children who underwent open reduction and IM fixation. In general, children who underwent closed reduction and casting had a decreased incidence of CS compared to those who underwent IM fixation; implicating the fixation method as a predisposing factor to CS. Furthermore, the authors found that children with longer fluoroscopy and operative times were also at increased risk for CS. In essence, the results of this study implicate that repeated and closed passes of IM fixation devices (i.e., flexible nails) can create soft tissue damage and swelling, creating a favorable environment for the development of CS. This is a recognized iatrogenic risk seen with this technique [12].
Although prior studies in the literature have not directly examined the risk factors for CS after flexible nailing of tibia fractures, the incidence in literature has ranged from 0.0 to 32.0% [8, 11, 21, 22]. Yet, it is unclear in these studies if CS occurred before or after flexible nailing. The higher rate of compartment syndrome associated with flexible nailing is in contrast to that reported for statically, locked reamed nails. Court-Brown et al. reported that 8.3% of their skeletally immature patients treated with reamed, statically locked nails developed CS [20].
In our series, we identified three factors associated with the development of CS after flexible nailing of tibial shaft fractures: weight greater than 50 kg, comminuted/complex fracture patterns, and presentation with pre-operative neurologic deficits in the absence of compartmental swelling.
There have been multiple studies in the literature, which have shown difficulties with treating older, heavier patients with flexible nailing (both in the femur [15] and the tibia [10]) particularly in patients who weigh above 50 kg. In fact, several authors have postulated that the relatively high incidence of CS that occurs with increasing age and size is due to muscle hypertrophy; particularly at the end of skeletal growth [17, 21]; the risk being related to the increased forces needed to perform a fracture reduction and nail fixation. However, in our cohort, the mean age of children with CS was 12 years old, and these patients likely had increase in adipose tissue resulting in their greater body weights, rather than the proposed increase in adolescent skeletal muscle. Either way, it appears that clinicians should be cognizant that patients over 50 kg who undergo flexible nailing are at significant risk for the development of CS (Figs. 5, 6).
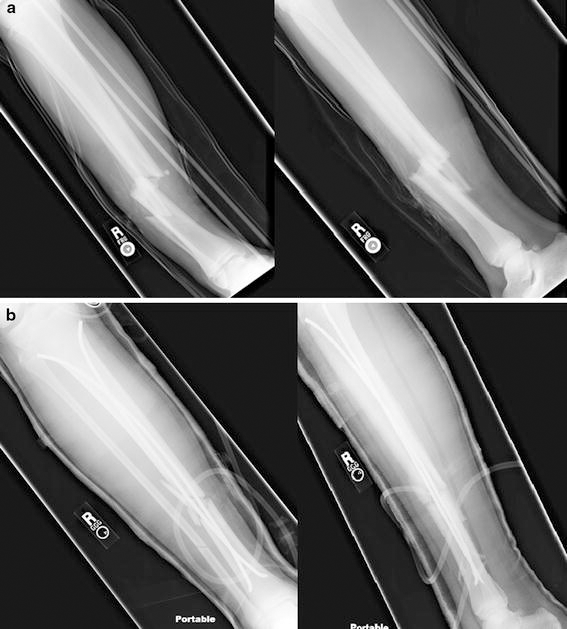
14 + 7-year-old, 65-kg boy with a right comminuted tibia fracture with motor weakness and decreased deep peroneal and superficial peroneal nerve function pre-operatively who developed CS 36 h after flexible nailing.
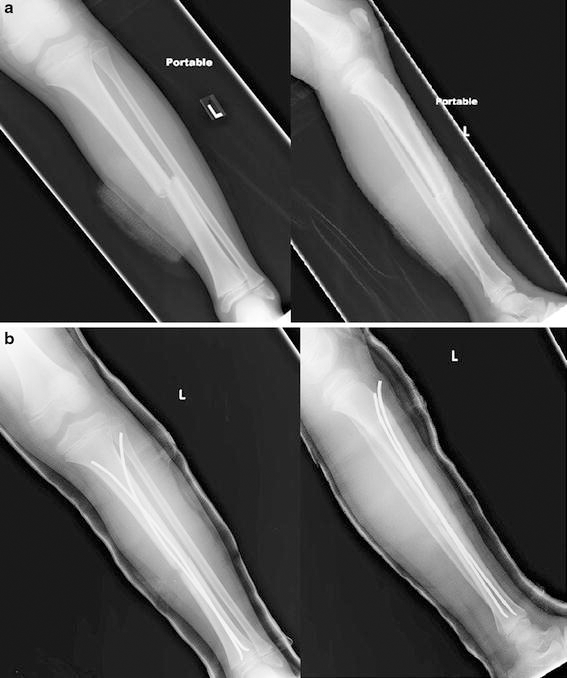
9 + 7-year-old, 31-kg boy with a left transverse tibia fracture without any pre-operative neurologic deficits who did not develop CS.
The second risk factor involves the difficulty with utilizing flexible nails for complex/length unstable fracture patterns, which has also been well documented in the literature [16, 34]. Not only do these fractures patterns indicate that a higher degree of energy was transferred to the limb during the injury, but they also present a more challenging fracture pattern to successfully achieve fixation with flexible nails. Flexible nails provide internal elastic support that relies on an envelope of relatively intact soft tissue and bone to provide counter support and guidance for fracture reduction and stability. Not only do these fracture patterns have increased risk for violation of that soft tissue envelope, but the more complex fracture pattern can result in an increased number of failed attempts to pass the flexible nail, injuring the soft tissue envelope even further. In addition, many of these fractures can also be shortened, and as the bone is brought out to length, there can be an increase in the compartmental pressure. As a result, clinicians should therefore use caution when utilizing flexible nails in these fracture patterns as nail passage may be difficult in an already compromised soft tissue environment (Figs. 5, 6).
Finally, we found that children with pre-operative neurologic deficits in the absence of compartmental swelling were more likely to present with CS. This may also be a marker of soft tissue damage, as there is a certain degree of soft tissue damage needed to result in compromised neurologic status. As a result, flexible nail fixation with multiple failed passes, as described previously, may be the final impetus to cause CS. Of note, these patients should not be considered as a group of patients who had CS prior to flexible nailing (particularly as 2 patients in the non-CS groups also had pre-operative neurovascular deficits). As mentioned previously, if patients presented pre-operatively with increased pressure/swelling in a compartment, paresthesias/anesthesia, paresis/paralysis, pain with passive stretch, intact pulses, and a “pink” extremity (the signs and symptoms of compartment syndrome; Fig. 1) [24], they were not taken to the operating room for flexible nailing as they were diagnosed with compartment syndrome. If patients presented pre-operatively with only a few of the aforementioned signs (particularly paresis, pain with passive stretch, or paresthesias) in the absence of compartmental swelling, the signs and symptoms were attributed to the inciting trauma rather than compartment syndrome. As Mubarak et al. have noted, swelling and palpable tenseness in a compartment are the first signs of compartment syndrome, with paresis and pain with passive stretch in the absence of compartmental swelling likely due to pain from the trauma rather than from a compartment syndrome [24].
Of the 4 patients who had pre-operative neurologic deficits that developed CS, all had soft compartments pre-operatively with 2 having only isolated muscle weakness (not frank paralysis) that was felt to be due to the trauma itself/pain from the injury. The other 2 patients also had soft compartments with decreased sensation globally in the lower extremity (deep peroneal, superficial peroneal, and tibial nerve). We believe that this may have represented a slight baseline increase in the normal compartmental pressure in the patients affected compartment stemming from the trauma, with the lower extremity subsequently “pushed” into CS from the flexible nailing. As a result, families with children that present with moderate neurologic symptoms pre-operatively should be watched very carefully for CS and the subsequent need for fasciotomies (Figs. 5, 6).
Interestingly, when we looked at our mechanisms of injury and divided them into high-energy (i.e., MVC, peds vs. bike) and low-energy (falls, sporting injuries) mechanisms, we found no difference in the development of CS. This was also true for polytrauma status, a surrogate marker for high-energy injury mechanisms. Erdos et al. examined trauma-associated acute CS of the lower extremities in 24 children. They found that fractures were the inciting cause in 71.0% percent of patients with a mix of high-energy and low-energy trauma causing CS in children from age 2 to 14 [32]. Grottkau et al. examined children with CS and also found that the most common mechanism of injuries was a mix of high-energy (ped vs. MVC 28.2%) and low-energy (falls, 13.7%) trauma [18]. Finally, in a series of flexible nailing presented by Srivastava et al. (who examined 24 tibia shaft fractures treated with flexible nailing), one of their cases of CS was a low-energy trampoline injury [11]. As a result, mechanism of injury, in isolation, does not establish a risk of CS after flexible nailing, but rather it is the extent of damage to the soft tissues around the tibia.
Further, we found that delay in treatment, prior closed reduction attempts, or method of reduction (open vs. closed) in the operating room did not differ between patients who did and who did not develop CS. This implicates the “actual” process of flexible nailing as the cause of compartment syndrome in our patient population rather than other confounding factors. In addition, we found no difference in the rates of CS between open and closed fractures. The rate of CS in adults has been noted to be between 6 and 9% in open tibial fractures [35, 36], which is in contrast to data of the pediatric population. Cullen et al. examined 83 children with open tibia fractures and found a 2.4% incidence of CS [37]. Irwin et al. examined 58 open tibia fractures and found a 1.7% incidence of CS [38]. Hope et al. examined 92 open tibia fractures and found a 4% incidence of CS [39]. It is important to note that none of these series cited treated their open injuries with flexible nailing. When the decision is made by the surgeon to treat an open pediatric tibia fracture with a flexible nail, the risk of CS developing is no different for open or closed injuries.
There are several weaknesses in our study. We did not obtain both pre- and post-nailing compartment measurements in our patients to determine the rise in pressure after nailing and/or determine whether there was a slight increase in the baseline pressure (within normal limits) in patients with pre-operative neurologic deficits with soft compartments. Second, we were unable to ascertain from the operating room records number of attempted nail passages that the surgeons made when flexible nailing their tibia fractures. Third, we had a relatively small number of treated patients over a 7-year period with multiple surgeons and fellows performing the procedure; thus, the absolute number for any one surgeon was quite low for this challenging surgery. As a result, we could not find a difference between our two groups in regards to total fluoroscopy time and total operative time (particularly to use as a proxy for a more difficulty surgery with repeated IM nail passes), as the experience of each surgeon greatly varied particularly in regards to operating speed and dependence on fluoroscopy. This is in contrast to the study by Yuan et al. who had over 80 patients who underwent IM fixation of their forearm fractures and was able to find an increased risk of compartment syndrome with increased fluoroscopy time and operative time [23]. We do believe that as the number of patients who undergo flexible nailing increases, increased fluoroscopy time and operative time will become markers of more “difficult” fractures rather than markers of surgeon's comfort level and experience with the technique itself.
Finally, some would argue that our method and criteria utilized to diagnose compartment syndrome is not the best method. We utilized an absolute pressure measurement under anesthesia (with a slit/wick catheter set-up) in any compartment greater than 30 mm Hg in lieu of utilizing a delta P (diastolic pressure or mean arterial pressure minus compartment pressure) value [24, 25, 40]. Staudt et al. examined normal compartment pressures of the lower leg in children and found that mean arterial pressure did not relate to age or pressure in the compartment (in contrast to delta P) and that children and adults have different resting pressures [25, 33]. In addition, as previously stated, delta P measurements are difficult to interpret due to anesthesia induced hypotension.
In conclusion, we recommend that children who are greater than 50 kg, have comminuted/complex fracture patterns, or have presenting neurologic deficits (i.e., particularly paresthesias or muscle weakness) in the absence of compartmental swelling should be monitored very closely for the development of CS after flexible nailing. Although we do recommend prophylactic fasciotomies if clinically indicated, compartment pressure measurements should be taken to assess for increased compartmental pressures after flexible nailing within the operating room, and fasciotomies done when indicated. Although an excellent option for the treatment of pediatric tibia fractures, surgeons should be aware of the risk of compartment syndrome after flexible nailing.
Footnotes
We have no conflicts of interest or funding sources to report.