
Abstract
Abstract
Background
The treatment of late-presenting developmental dislocation of the hip (DDH) is still controversial. A consecutive series of 32 patients not previously treated (43 hips, Tönnis grade 3 or 4) underwent progressive closed reduction followed immediately by innominate osteotomy between 1964 and 1976. They were between 1.5 and 5 years old at the time of pelvic osteotomy. This study was designed to check the outcome of these patients more than 30 years later.
Methods
Eight patients living outside of France (North Africa) could not be reached and one patient had died of an unrelated cause. The remaining 23 patients (32 hips) were reviewed with clinical assessment (Merle d'Aubigné, Harris and Western Ontario and McMaster Universities Osteoarthritis Index [WOMAC] scores) and anteroposterior (AP) pelvic radiograph. This represents a 75% rate of follow up at 31 to 44 years post-operatively.
Results
In two patients, surgery was repeated due to residual subluxation. Only one patient needed a total hip replacement (THR) 33 years after initial treatment. The Merle d'Aubigné, Harris and WOMAC scores for the surviving hips were excellent or good in almost 80% of the cases. In four cases, radiographic signs “at risk for” osteoarthritis were present. Regularity of the femoral head was perfect in seven hips, regular in 18 and irregular in six. According to the Severin–Seringe classification, 25 hips could be classified as group I (14 group IA and 11 group IB), three group II and three group VII.
Conclusion
The long-term results of non-previously treated late-presenting DDH by the technique of progressive closed reduction followed by innominate osteotomy are quite good and compare favourably with the long-term results of open reduction with the same osteotomy.
Introduction
In spite of screening programmes to detect developmental dislocation of the hip (DDH), we still come across cases which are diagnosed after walking age. The treatment of such late-presenting cases is more difficult with less predictable prognosis. Ideally, one should undergo a concentric and stable reduction, correct the hip dysplasia and avoid avascular necrosis (AVN) in order to obtain a concentric hip with a regular femoral head and a well-developed acetabulum at the end of the growth period. There are various modalities of treatments described and some are still controversial, especially the method of reduction of the femoral head inside the socket. Open reduction is considered by many teams as the “gold standard” [1]. At our institute, we are using for more than 40 years “an atraumatic progressive orthopaedic reduction” technique for late-presenting DDH [2]. In order to correct the acetabular dysplasia, it was proposed to complete the reduction by femoral or pelvic osteotomies [3, 4]. We use in our institution Salter's innominate osteotomy after this orthopaedic reduction.
Although short-term results are important to assess the immediate success and complication, the results at the end of the growth period [1, 5] and, above all, long-term results should be taken into account [6]. In this study, we have included those cases diagnosed in walking age children below the age of 5 years and previously untreated. This study was designed to analyse the results of our method of treatment into middle age with a minimum of 30 years of follow up.
Materials and methods
Patients
The present study is a retrospective review of a prospectively assembled cohort. The senior author (GM) has prospectively collected data on all patients with DDH treated by innominate osteotomy between the years 1964 and 1976. A total of 190 innominate osteotomies were performed by the senior author in 139 patients during this period.
We have included in our study the patients with a primary progressive reduction performed in our institution, for DDH grade 3 or 4 of Tönnis [7], with an age at the time of the innominate osteotomy of between 18 months and 60 months, and a minimum of 30 years of follow up. There were 55 hips in 41 patients with these criteria. We have excluded those cases with any previous hip surgery or any previous attempt of closed reduction made at another institution (ten hips in seven patients) or in case of failure of the primary progressive reduction which necessitate an open reduction (three hips in two patients). Thus, 42 hips in 32 patients (28 females and four males) had the potential to be included in our study.
Treatment programme
This method has been previously described by the senior author [2]. The steps in this treatment method are: (1) to apply a progressive traction to lower limbs so that the femoral head lies opposite to acetabulum; (2) to apply a hip spica and wait for the spontaneous penetration of the femoral head through the acetabular labrum; (3) to correct the acetabular dysplasia by Salter's osteotomy (Fig. 1a–e).
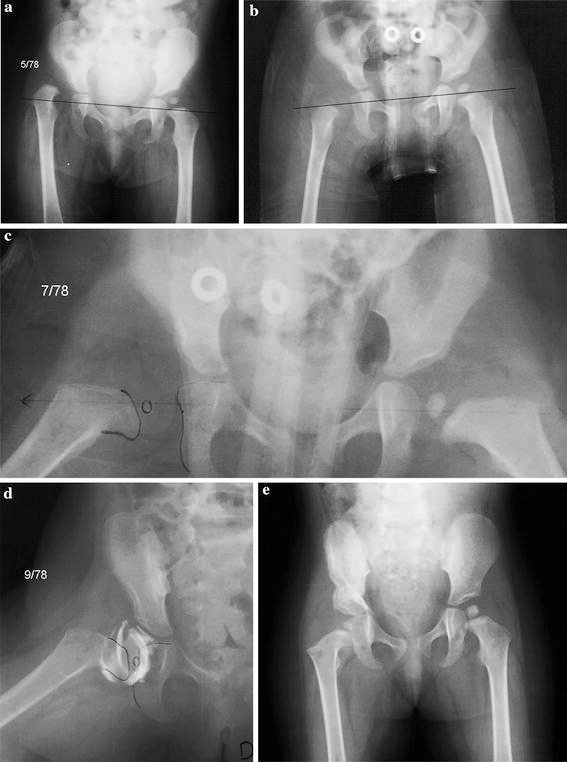
The traction is very progressive and longitudinal in the horizontal plane, in order to bring the epiphysis up to the reduction axis, which is the line passing through the centres of the two teardrops (Fig. 1a). Adhesive skin traction is applied on both lower limbs and is carefully padded with bandages. The bandages are rerolled every second day in order to keep the limbs under tension and to avoid skin problems. Counter-traction is obtained by immobilising the chest of the child in a canvas brace fastened to the bed and by elevating the bottom part of the reduction frame. For an 18-month-old child, we usually start the traction on both sides with 0.5 kg and progressively increased to 3–4 kg by the end of the second week. Anteroposterior (AP) X-ray of the pelvis is performed at this time to check the lowering of the upper femur (Fig. 1b). If the epiphysis seemed to be in front of the acetabulum, then we begin the abduction to make the femoral neck horizontal. This is performed by lateral displacement of the traction pulley on the curvilinear edge of the reduction frame. An abduction of 45–50° is achieved within 8 days and, finally, internal rotation is applied to neutralise the femoral anteversion. This angle was measured using an X-ray biplanar method, which may be considered as a modified Magilligan's method [8, 9]. The medial rotation is performed thanks to a folded strap applied at the base of the thigh and supporting the weight progressively increased up to 1 kg. It takes another 1 week to neutralise the femoral antetorsion. It is useful in order facilitate the medial rotation to decrease the traction weight. At the end of this period of traction (4 weeks for the youngest child, 8 weeks for the oldest) a second AP X-ray is performed at this time. It must show the totality of the femoral neck well positioned on the reduction axis (Fig. 1c). A double hip spica cast is then applied, under general anaesthesia, in the same position, which means with the legs in extension abduction and medial rotation, without any testing or reduction manoeuvre. At this time, an AP X-ray in the cast shows the good positioning of the upper femur but the epiphysis is far away from the acetabulum. Spontaneously, the heads gets reduced. At the beginning of the experience, patients spend at least 2 months in the cast before checking the reduction by an arthrography (Fig. 1d). But it appears now that 1 month is enough, as attested on the AP X-ray by the overlapping of the epiphysis with the posterior column. The cast is then removed to perform Salter's osteotomy, as described by Salter [1], with only slight modification: maintaining the position of the legs in abduction and medial rotation from the time when the “reduction cast” is removed to the time when the “osteotomy cast” will be made, no adductor tenotomy, no opening of the hip joint nor capsulorrhaphy, two unthreaded K-wires to stabilise the osteotomy and a bilateral spica cast for 6 weeks. This was followed by pins removal and immobilization for a further 2 months with an abduction splint (Fig. 1e).
Finding the patients after 30 years
The most difficult task in this study was to locate these patients after 30 years. Most of them have moved to other cities, and most of them were females and have changed their names after marriage. French national health insurance does not give information of the new addresses of their members. Somehow, we were able to contact the relatives or general practitioner of the city where they lived at the time of the treatment programme. Most of the time, we had to check the records office of the patients’ hometown. We also searched for them using telephone directories and social network sites.
Clinical and radiological assessment
The complete clinical and radiological records of the patients at the time of the initial treatment until the end of the growth period were studied.
Each of these patients readily agreed to return to “Institut Calot” for review and clinical examination performed by the first and second authors based on the original Harris hip score [10] and the original Merle d'Aubigné score [11]. According to the original Harris score ranging from 0 to 100, an excellent hip has 90–100 points, good 80–89 points, fair 70–79 points and bad 70 points or less. According to Merle d'Aubigné score ranging from 0 to 18, an excellent hip has 17 or 18 points, good 15 or 16 points, fair 13 and 14 points, and bad 12 points or less. Patients completed also the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) questionnaire for hips [12], with 0 points for a perfect score and 100 points being the worst score.
We had an AP radiograph of the pelvis at the final follow up to study:
The centre-edge angle of Wiberg (CE), which is considered as “normal” if it is more than 25°, “abnormal” less than 20° and “borderline” between these limits [13] The shape of the femoral head with the method of Mose, the head being “normal” if its outline is covered by the same circle of the template, “regular” if its outline is in a zone limited by two concentric circles (2 mm), “irregular” in the zone limited by three concentric circles (6 mm) and “very irregular” in the zone limited by four or more concentric circles (≥8 mm) [14] The minimum joint line (articular space) with a cut-off of 2 mm to indicate an osteoarthritis [15] The Kellgren–Lawrence classification for osteoarthritis into five grades, 0 none, 1 doubtful, 2 mild, 3 moderate and 4 severe [16] As proposed by Severin [17] and modified by Robert and Seringe [18], we classified the hip at skeletal maturity into nine groups, IA perfect hip with normal or regular femoral head and CE > 25°, IB normal femoral head but borderline CE, IIA and IIB with irregular femoral head and CE normal or borderline, respectively, III being dysplastic with CE < 20°, the femoral head being normal, regular or irregular, IV residual subluxation, V residual dislocation, VI femoral head very irregular and VII osteoarthritis
Statistical analysis
Statistical testing and survival analysis were performed by a trained statistician. For the survival analysis, total hip replacement (THR) is considered as a failure, not the patient's death from unrelated causes. Survival time was calculated from the date of the innominate osteotomy to the last follow up examination or the date of the THR.
The Mann–Witney U statistical test was used for Tables 1 and 2 and Fisher's exact test was used for Table 3 (Statistica 9.0). A very significant difference was noted for a P-value < 0.01.
Clinical and radiological presentation of the series
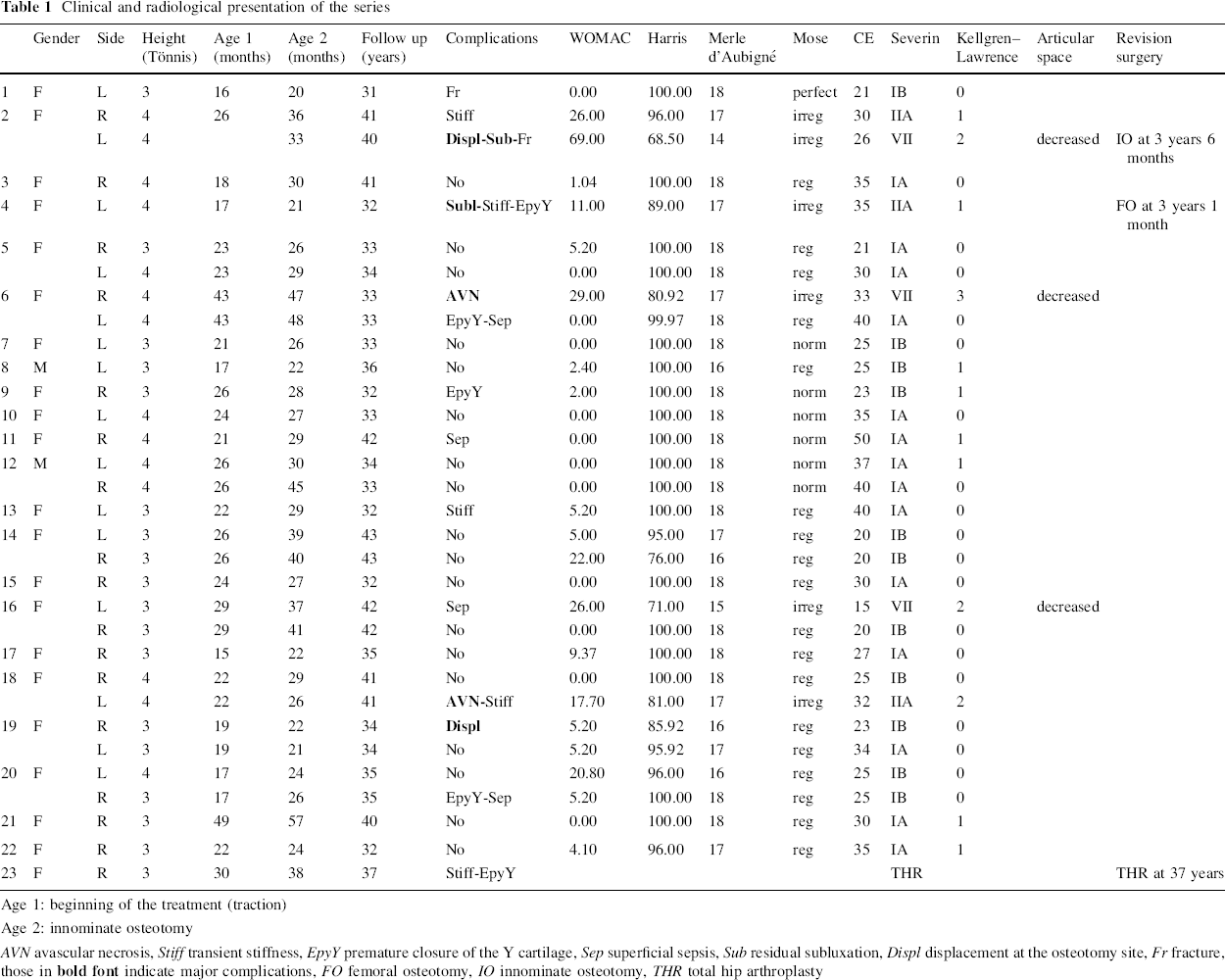
Age 1: beginning of the treatment (traction)
Age 2: innominate osteotomy
AVN avascular necrosis, Stiff transient stiffness, EpyY premature closure of the Y cartilage, Sep superficial sepsis, Sub residual subluxation, Displ displacement at the osteotomy site, Fr fracture, those in
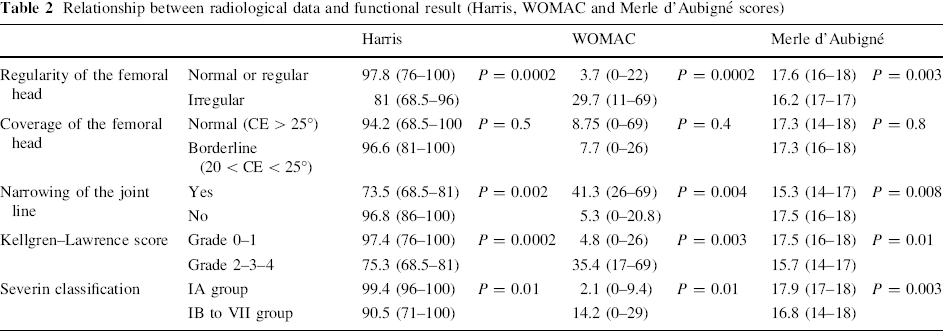
Relationship between radiological data and functional result (Harris, WOMAC and Merle d'Aubigné scores)
Relationship between complications and functional result

Results
Eight patients (nine hips) born in a foreign country (mainly Algeria) and who returned to their native country at the end of the treatment could not be traced. One patient (one hip) died at 23 years of age of unrelated causes. At the end, we were able to contact and review for clinical and radiological examination 23 patients (32 hips) out of 32 patients (42 hips) in the initial cohort, with a follow up rate of 72% (75% hips) (Table 1).
There were 21 females and two males, among which nine patients had bilateral DDH. There were 17 right and 15 left DDH, 18 were of Tönnis grade 3 and 14 were grade 4. The mean age at the time of Salter innominate osteotomy was 31 months (range 20 months–4 years 9 months) and the mean age at the beginning of the traction was 23 months (range 16 months–3 years 7 months). In two cases, it was necessary to perform a femoral derotation osteotomy along with pelvic osteotomy for wide anteversion (55 and 60°).
Complications occurred in 12 out of 23 patients. Post-operative minor complications occurred in nine patients and included fractures around the knee (2), transient stiffness (5), superficial sepsis around the K-wire (4) and premature partial closure of the Y cartilage (5). Post-operative major complication occurred in five patients and included AVN of the femoral head (2), displacement of the innominate osteotomy (2), with residual subluxation (2). In these cases, it was necessary to complete later on the treatment programme with a femoral osteotomy in one case and a triple pelvic osteotomy in the other case.
At the end of the growth, four patients (five hips) could not be reviewed. For the remaining 27 hips, there were 21 Severin group IA, two Severin group IB, three Severin group IIB one Severin group III hips.
Survival analysis
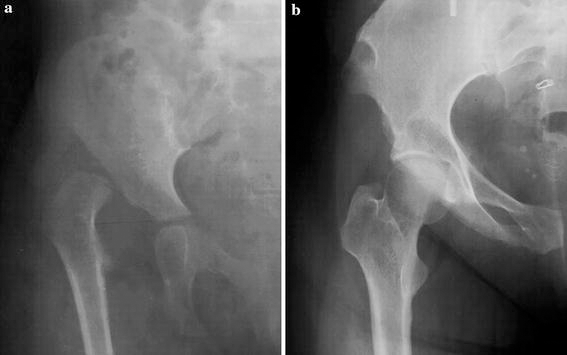
The mean length of follow up for patients still alive at the end of the study was 37 years (range 31–44). Average age of the patients at this time was 39 years (range 33–46). Only 1 patient underwent a THR 33 years after initial treatment with the histological diagnosis of AVN of the femoral head (Fig. 2). Thus the rate of THR in the 23 patients surviving more than 30 years after the treatment programme was 4%. The only failure occurred 33 years after the treatment programme, The data became unreliable after 40 years of follow up. Up to that time, the survival rate is 95.2% (95% confidence interval, 77.3–99.2%)
Clinical results
A total of 31 hips in 22 patients did not require replacement at the last follow up. Score rating has been used for these surviving hips. The average Harris score was 94.5 (range 68–100), with 24 excellent results, four good results, two fair results and one bad result. The average Merle d'Aubigné score was 15.6 (range 14 to 18), with 25 excellent results, five good results, one fair result and no bad results. The average WOMAC score was 8.7 (range 0–69).
Radiological results
The average CE angle was 29° (range 15–50°). It was considered as normal in 18 hips, abnormal in one hip and borderline in 12 hips. The shape of the femoral head was normal in seven hips, regular in 18 hips, irregular in six hips and none were considered as very irregular. A narrowing of the joint line was present in three hips, and Kellgren–Lawrence scoring of osteoarthritis showed mild signs of osteoarthritis in three hips and moderate signs in one hip.
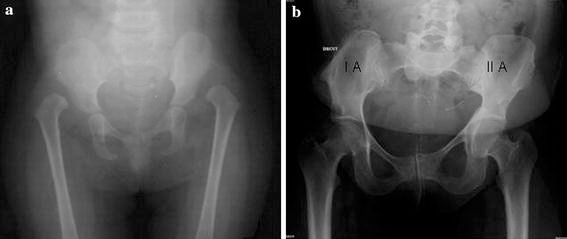
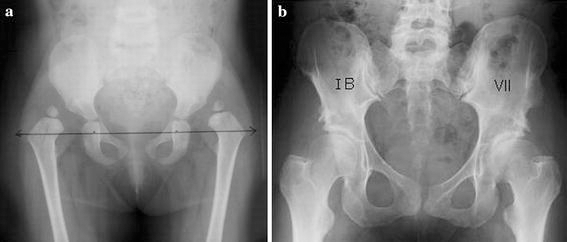
According to the Severin classification modified by Robert and Seringe, 14 hips are in group IA (Fig. 3), 11 hips in group IB (Fig. 4), three hips in group IIA (Fig. 3) and three hips in group VII (Fig. 4). When we compared theses results to the results of the classification made at the end of the growth period by another observer, we found that 12 hips stayed in the same group, seven hips changed from IA to IB, three changed from IA, IB and IIB to VII, one hip changed from IA to IIA and three improved their group by changing from IIB to IIA and from III to IB.
Clinical and radiological relationships
As far as the regularity of the femoral head is concerned, the Harris, Merle d'Aubigné and WOMAC scores are significantly better for the normal or regular femoral heads than for the irregular femoral heads. If we consider the CE angle, there is no difference in the Harris, Merle d'Aubigné or WOMAC scores in hips with borderline CE angle and hips with normal CE angle. Narrowing of the joint line and Kellgren–Lawrence score are very well correlated with fair or bad results appreciated by the Harris, Merle d'Aubigné or WOMAC scores. In a “perfect hip” as when we considered the Severin IA group, the Merle d'Aubigné score and, to a lesser extent, the Harris or WOMAC scores are better than in the other Severin groups (Table 2). Only major complications occurring during the treatment programme affect significantly the functional result (Table 3). It appears that the complications occurring during the treatment are significantly related with results which are not perfect and also with some irregularity of the femoral head and, on the other hand, hips without complications are always with normal or regular femoral heads and are always in Severin groups IA or IB (Table 4).
Relationship between complications, Severin classification and shape of the femoral head

Discussion
Long-term results are necessary in order to assess the efficiency of treatment for DDH. Hip problems in adult life such as osteoarthritis are expected in case of residual deformities, including incongruency of the hip joint, acetabular dysplasia or loss of sphericity of the femoral head. These hip problems tend to worsen with growth and it is mandatory to follow these patients to skeletal maturity. It is usually sufficient to predict the fair or poor results in adult life in case of substantial deformity at the end of the growth period, but this follow up is too short when the deformity is mild and some series have shown deterioration of the condition 30 years after the initial treatment. This is the reason for our study.
Undoubtedly, the final outcome is dependent upon the age when the treatment of DDH was begun and better results are expected when the treatment was started before walking age. In the late-diagnosed cases, concentric reduction is more difficult to obtain, with higher risk of AVN of the femoral epiphysis and less possibility of spontaneous correction of the acetabular dysplasia. In 1958, Robert Salter described his technique of open reduction and innominate osteotomy for the treatment of late-presenting DDH [4]. This technique is still considered in many countries as the “gold standard”. The results of short-term and long-term follow up of his technique were published and considered as references. In France, although Salter's osteotomy is a very well accepted method of correction of the acetabular dysplasia, many teams were still using the technique of progressive closed reduction developed in France by Petit and Morel. Not opening the joint was considered by them as a major point to avoid growth disturbance in the hip, especially for the femoral head.
The aim of the present study is to assess with a long-term follow up of 30 years or more if such an assertion could be confirmed. We decided to include in our series those patients treated at walking age and those under 5 years of age at the time of the treatment, as they correspond to what we see now in our country. We have excluded the patients who were previously treated, as they present a completely different challenge, with difficulty in comparing the complications of our treatment or of the initial management. In order to obtain a homogenous series, we have included only the true dislocated hips where the difficulty of the treatment is the major concern.
From the time where our first patient was included in 1964 to the last patient in 1976, we used the same method of treatment. The reduction is achieved by progressive traction in the horizontal plane to place the femoral head opposite the acetabulum. It is not just traction to “stretch” the soft tissues in the provision of a closed or open reduction as it is used by some teams to prevent an ischaemic problem, but it is traction to place the femoral epiphysis with the best orientation and as less obstacles as possible in front of the acetabulum. To do that, the traction is applied first in the neutral position to pull the femoral head below the limbus in order to avoid its invagination when the abduction is started. The degree of abduction and then the degree of internal rotation are defined in relation to the degree of inclination and anteversion of the femoral neck, previously measured by the radiographic method. The reduction occurs by itself spontaneously in the cast. At no time and under no circumstances is a forceful manoeuvre applied to facilitate the reduction, or even to test it.
From the earlier days of the series, we use pelvic osteotomy to treat the acetabular dysplasia because a femoral procedure alone, even in early childhood, does not provide sufficient remodelling. We perform the innominate osteotomy like it was described by Salter, as soon as the concentric reduction is achieved. This was confirmed in the earlier days by arthrography but, after gaining some experience with this technique, nowadays, only an AP radiograph is needed. Reduction is confirmed by the overlapping of the femoral epiphysis on the posterior column of the pelvis. Some surgeons prefer to perform the pelvic osteotomy at a later stage if the acetabular dysplasia does not correct by itself. There are few cases where such a spontaneous improvement of the acetabular dysplasia can occur, but they are probably infrequent when the treatment of a true DDH is started after walking age. Some other kind of pelvic osteotomies have been described to treat the acetabular deficiency. We do not have any experience with them in DDH and they need to be studied with a long-term follow up in order to be compared with Salter's osteotomy. Capsulorrhaphy was not used at the time of Salter's osteotomy, as we did not find it necessary for the stability of the reduction if it was really concentric. But a careful positioning in the cast after the surgery is needed and we recommend the use of an abduction brace after weaning off the cast for a period of 2 months. Femoral osteotomies with some shortening, which are frequently needed in cases after 5 years of age or after the failure of previous treatment, were never performed in our series, where the progressive traction was able to bring the femoral head into the correct position without any undue tension. In only a few cases was a derotation osteotomy performed for excessive femoral anteversion.
Failures to reduce the dislocated hip happened in 5% of the cases and were excluded from the long-term study, as they required an open reduction. Such failure of reduction may also be seen with the same rate in series of open reduction. Redislocation or residual subluxation occurred in our series in two cases, due to displacement of the innominate osteotomy. They were treated with closed reduction or re-osteotomy, but did not require open reduction. For this reason, they have been included in the series for the long-term results.
The occurrence of AVN is thought to be the worst complication causing deformity of the femoral head and subsequent osteoarthritis. AVN occurred in two patients (6%) of this study group. In a previous series in which the dislocated and subluxed hips were included, we found only a 4.4% occurrence rate of AVN [5], and an even lower rate of 3.3% when dysplastic hips were added to the series [19]. The Saint Vincent de Paul team who uses the same technique of reduction found an even smaller number of AVN, but, in their series, subluxed and dislocated hips were mixed [20]. Our rate of 6% of AVN is favourable compared to the complication rate with open reduction for true dislocation of the hip.
Twenty-three of the 32 patients in the initial cohort were reviewed with a follow up of more than 30 years. It corresponds to a follow up rate of 72%. If we take into account only the patients born and still living in France, there were 23 out of 25 in the initial cohort who were reviewed and the follow up rate in this case is 92%. Even if our series is not the largest reported, it has the advantage of being very homogenous, with very few patients having been lost.
Long-term results were studied in two ways. First, we analysed the number of hips in the study group which were replaced by arthroplasty. It was shown in Thomas et al.'s series [21] that the first failure in the treatment of late-presenting DDH treated by open reduction and Salter osteotomy happened 30 years after the initial procedure with a progressive increase in the number of failures with time. At 45 years of follow up, the survival rate is 54%. In our series, even if we do not have exactly the same follow up, we did not find such a rate of failure. We have only one hip which underwent replacement, and this failure may not be completely related to the initial problem. No decrease in the survival rate was observed and, at 40 years of follow up, the survival rate is still the same (97%) as it was at 35 years.
Secondly, we have studied for the surviving hips the clinical and radiological results. The vast majority of the surviving hips have good or excellent clinical results as far as the WOMAC, Harris and Merle d'Aubigné scores are analysed. Signs of osteoarthritis on the X-rays are present in only four hips. Regularity of the femoral head, coverage of the femoral head by the acetabulum and the joint space in the frontal plane were used for the Severin classification. Eighty percent of the hips were in class I and almost 50% of the hips were perfect (class IA). These results are better than those described in Thomas et al.'s series of open reduction, with the majority of surviving hips being in class II. This difference is due to the presence of some irregularity of the femoral head in the “open reduction group” in comparison to our series, where most of the femoral heads are normal or regular at the last follow up.
The shape of the femoral head seemed to be a major factor of prognosis, with a good correlation with the clinical result at the last follow up. It does not seem to change with time, most of the regular or normal femoral heads at the end of the growth are still regular or normal femoral heads at the last follow up and, of course, irregular femoral heads at the end of the growth period did not improve with follow up.
To have a normal or a borderline CE angle does not seem to be a very important factor for the prediction of the prognosis. Thanks to innominate osteotomy, very few hips are seen at the last follow up with a dysplastic acetabulum.
Major complications during the treatment programme, especially AVN and displacement of the innominate osteotomy with residual subluxation, is a factor which may explain some of the fair results in our series.
Even if retrospective studies are unsatisfactory, the fact that more than 30 years later the vast majority of the patients treated for DDH between walking age and the age of 5 years did well with their hips not being replaced and with no reason to worry about premature osteoarthritis is a strong argument to recommend progressive orthopaedic reduction rather than open reduction. For us, this is the best way to avoid growth disturbance of the femoral head, which will lead many years later to premature osteoarthritis and, subsequently, THR.
Footnotes
Acknowledgement
We thank Stéphane Bouilland, PhD, Engineer at the Berck Institute for Disability, for his assistance in the statistical analysis of the data.