
Abstract
Purpose
To describe the demographic and clinical characteristics of children who presented with open femur fractures.
Methods
A retrospective chart review of all children treated for open femur fractures at the McGill University Health Center between 1980 and 2009 was conducted. Thirty-seven patients (28 males and 9 females) were identified. Union was determined clinically by the absence of pain, tenderness to palpation and crepitus with motion. Complications were reported.
Results
The mean age of the patients was 11.5 years (range 2.8–18.1 years). The mechanism of injury involved motor vehicle-related injuries in 70% of cases. There were 13 Grade I, 15 Grade II and 9 Grade III fractures. The treatment involved traction and hip spica in 11 patients, external fixator in nine patients, intramedullary nailing in seven patients, open reduction and internal fixation in six patients, and traction and an ischial weight bearing brace in four patients. Average time to union was 5.1 months (range 1.5–14.4 months). Infections occurred in ten patients, nine had delayed unions, two developed malunions, four had a refracture and four patients developed a limb length discrepancy >2 cm.
Conclusions
Open fractures of the femur are often accompanied by associated injuries, indicating the importance of early and comprehensive treatment. Treatment may include hip spica application in school-age children and solid intramedullary nails in adolescents. In children with multiple injuries, specifically those with higher fracture grades, treatment with an external fixator provides immediate stability of the fracture and allows early mobilization and ease of management of associated injuries.
Keywords
Introduction
The incidence of femur fractures in children is 1.6% of all bony injuries [1]. Of these, 4% are open fractures [2] and are for the most part (90%) due to high-energy mechanisms [3]. Research has shown that the presence of associated injuries and complications is high in this type of fracture [2, 4–8] and proportional to the severity of the trauma [9]. Although the optimal method of fracture stabilization remains controversial [10], excellent functional results can be obtained with proper management.
There are many published reports on open femur fractures in the adult literature; however, only a few studies have specifically addressed open femur fractures in children [2, 10]. Several methods of treatment have been described in the management of these conditions, such as traction and hip spica, external fixator (EF), and intra-medullary (IM) nail. Up to the early 1980s, most femur fractures were treated non-operatively [11], including traction followed by casting, or immediate casting [12]. Medical advances have increased the availability of operative techniques for treating pediatric femur fracture, leading to early mobilization and a reduced hospital stay [13]. The IM nail is often used in the treatment of open femur fractures in adolescents and presents several advantages, including immediate mobilization, earlier return of function with less joint stiffness, short hospitalization and low cost. The disadvantages of this technique include risk for infection and the need for a second operation for rod removal [14]. In general, the IM nail has been found to involve fewer complications, refractures and malunions [10] and a faster healing time [2] than treatment with an EF, but the use of EF is indicated in children with open, high-energy and complex fractures [15–17] as well as with children with multiple injuries [17, 18]. The complications of EF may include refractures, pin tract infections and scarring [17, 19, 20]. Other forms of treatment may include traction and ischial weight bearing brace (IWBB) and open reduction with internal fixation (ORIF) [21, 22]. The choice of treatment in a specific case is based on several factors, including the patient's age, degree of wound contamination, presence of associated conditions, the preference of the surgeon and the availability of stabilization devices [14].
The purpose of this study was to describe the demographic and clinical characteristics of those children and adolescents who presented with open femur fractures and associated injuries. The association between age, gender, type of treatment, Gustilo grade and type of wound closure and time to union was explored.
Materials and methods
A retrospective case series was designed. Approval from the Director of Professional Services at the Shriners Hospital was obtained, in accordance with the guidelines provided from our Institutional Review Board.
Charts and radiographs of all children treated for open femur fractures at the McGill University Health Center between 1980 and 2009 were retrieved and reviewed by a chief resident (PA), a senior resident (VJ) and a medical student (SY). All open femur fractures were included regardless of location and mechanism of injury. Thirty-seven patients (28 males, 9 females; 37 open fractures of the femur) were identified at the time of the review.
A number of variables, including age, gender, mechanism of injury, Gustilo grade [23, 24], associated injuries, treatment, and mean time to follow-up, were recorded and are summarized in Table 1. An associated injury was defined as the presence of one or more fractures and/or injury to another body system other that skin lacerations and abrasions requiring medical attention.
Baseline characteristics
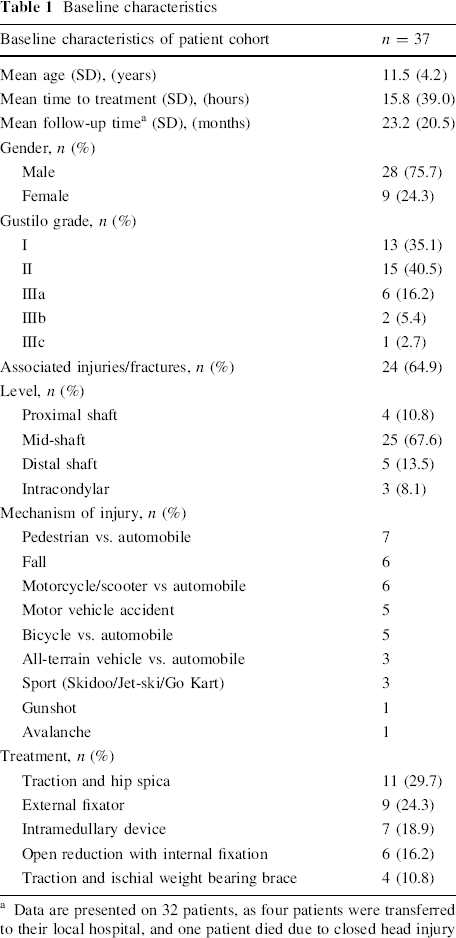
Data are presented on 32 patients, as four patients were transferred to their local hospital, and one patient died due to closed head injury
All patients were subjected to the trauma protocols of the time and investigated for any concurrent injuries. All fractures were initially splinted and antibiotics administered. Twenty-seven patients received a first-generation cephalosporin, three had the addition of gentamycin and two received a third antibiotic. Three patients received a second-generation cephalosporin, and two patients received a combination of two beta-lactams. All patients received tetanus prophylaxis. Thirteen patients underwent irrigation and debridement within the first 6 h. Lengthy delays were due to long travel time for patients from remote regions, and one patient with a delayed treatment of 10 days was injured on vacation and had been treated conservatively without antibiotics. The method of fracture stabilization was determined by the attending surgeon (RH).
Union was determined clinically by the absence of: pain, tenderness to palpation and crepitus with motion. The presence of adequate bridging callus formation was used for radiographic healing. Delayed union was defined as taking >6 months to unite. A non-union was judged to be present with the absence of the above criteria at the last follow-up.
Complications were reported for each patient and included infections, delayed unions, malunions, refractures and limb length discrepancies (LLD). Complications directly related to a fracture other than the open femur fracture were not included.
The association between gender and time to union was calculated using a t test. Pearson correlations were used to determine the association between age and time to union, and analysis of variance was used to calculate the association between categorical variables (Gustilo grade, type of treatment, type of wound closure) and time to union. Statistical analyses were conducted using SAS ver. 9.2 software (SAS Institute, Cary, NC).
Results
Demographics
The average age of patients was 11.5 years (range 2.8–18.1 years). The mechanism of injury was high energy in nature for all patients. Twenty-six (70.3%) of the patients presented with motor vehicle-related injuries, including pedestrian/car (7 patients, 18.9%), motorcycle/car (6 patients, 16.2%), bicycle/car (5 patients, 13.5%), motor vehicle accidents (5 patients, 13.5%) and accidents involving all-terrain vehicles (ATVs) (3 patients, 8.1%). Other injuries included falls (16.2%), sports-related injuries (8.1%), gunshot wound (2.7%) and an object falling onto a patient (2.7%).
There were 15 right and 22 left fractures. The location of the fracture in the femur was the proximal shaft (11%), the mid-shaft (68%), the distal shaft (13%) and intracondylar (8%). There were 13 Grade I fractures (35%), 15 Grade II (41%) fractures and six Grade IIIa (16%) fractures, two Grade IIIb (5%) fractures, and one Grade IIIc (3%) fracture (Table 1).
Fifteen patients (41%) had associated fractures, including eight who had multiple fractures of the lower limbs, upper limbs and spine; all had been involved in a motor vehicle-related injury. Three patients had a vascular injury (2 profunda femoral artery pseudo aneurysm, 2 superficial femoral artery tears), one had a neurologic injury (common peroneal nerve palsy), nine had intracranial injuries (6 contusion or concussion, 2 bleeds, 1 seizure), 14 had maxillo-facial injuries, four had thoracic injuries (1 tension pneumothorax, 3 pulmonary contusions), and two had abdominal injuries (all with multiple organ involvement requiring laparotomy and splenic removal). A 7-year-old female died within 48 h of her accident from a severe head injury. She was hit by a car as a pedestrian and had sustained multiple injuries to other systems.
Treatment management
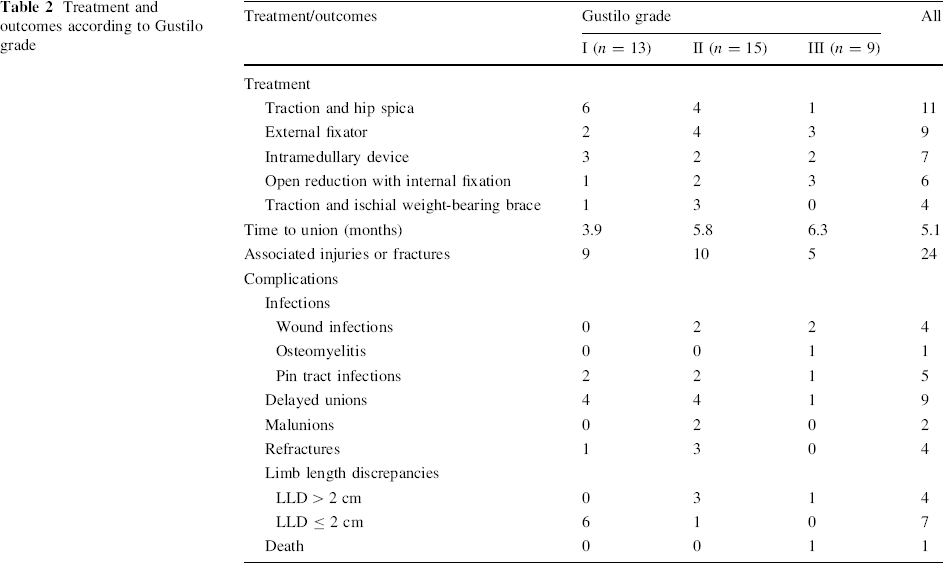
The average length of time before the open femur fracture was treated was 15.8 h (range 2.1–240.0 h), with 13 patients receiving orthopedic care for ≥10 h following their injury. Most of these patients were either living in the Northern territories or on vacation, in which case basic care, including antibiotic treatment, was initially provided, and they were then transferred to our institution. All 37 patients had initial irrigation and debridement surgery. Nine patients (24%) required a second debridement procedure, three (8%) underwent a third, and one (2%) required a fourth. All those who needed additional irrigation and debridement had a Gustilo grade of II (n = 4) or III (n = 5). Twenty (54%) of the wounds were closed primarily, with a mean healing time of 9.6 months (range 1.5–14.4 months), six (16%) were closed secondarily, two (5%) were delayed primary closures and eight (22%) underwent split thickness skin grafting. One patient died due to a closed head injury before wound closure was achieved. Treatment of the open femur fracture involved the use of traction and hip spica (11 patients), EF (9 patients), IM nailing (7 patients), ORIF (6 patients) and traction and IWBB (4 patients). ORIF and EF were used most readily for Grade III fractures, while traction and hip spica was most often used for Grade I fractures (Table 2).
Treatment and outcomes according to Gustilo grade
Time to union
Average time to union was 5.1 months (range 1.5–14.4 months). Mean union time in relation to patient age was 4.2 months for patients younger than 6 years, 5.5 months for patients between 6 and 12 years of age and 5.0 months for patients older than 12 years. These differences were not statistically significant (P = 0.69). Mean time to healing was 4.82 months for males and 5.42 months for females; there were threefold more males than females. Mean time to union was significantly shorter (P = 0.04) for Gustilo grade I fractures (mean 3.78 months) than for grades II and III fractures (mean 5.74 months). Healing time according to treatment was 7.2 months for EF, 4.7 months for IM nail, 4.2 months for ORIF, 4.3 months for traction and hip spica and 5.3 months for traction and IWBB. These differences did not achieve statistical significance (P = 0.26). The average follow-up time (based on data on 32 patients) was 23.2 months (range 3.0–77.5 months). Of the 37 patients, four received initial treatment, stabilization and debridement in our institution and then transferred to their local hospital for further follow-up, and one patient died from a traumatic brain injury within 48 h of receiving the injury.
Complications of treatment
Complications of treatment included infections, delayed unions, malunions, refractures and LLD. A 16-year-old girl who was injured in a pedestrian/car collision and who was treated with traction and IWBB had a pulmonary embolus. Another patient, a 14-year-old boy who had a scooter accident and was treated at our institution with an IM nail for his fracture 10 days after the injury, had toxic shock syndrome and acute respiratory distress syndrome and was transferred to the intensive care unit. Both recovered from these complications.
Infections
Infections occurred in ten patients (27.0%) and included osteomyelitis (1 patient), wound infections (4 patients) and pin tract infections (5 patients). All ten patients responded favorably to antibiotics. Regarding the four wound infections, two occurred in children treated with ORIF, one treated with EF and one treated with IM nail. One patient of the four who had a wound infection had a delayed healing of 9 months (treatment: EF) as a refracture occurred after the removal of EF. These data do not support a relationship between infections and wound healing. All five pin tract infections occurred in those with an EF. There was no deep wound infection.
Delayed unions
There were nine delayed unions, from which four patients were treated with EF, two with IWBB and four with traction/hip spica. Among these patients, an equal number (4 patients each) had Gustilo grades I and II fractures, respectively, and one had a Grade III fracture. All four children who had a refracture had a delayed union. All fractures eventually united; there was no case of nonunion.
Malunions
There were two patients who developed malunion of their fractures. The first patient was a 7.1-year-old male who sustained a Gustilo grade II open left femoral fracture of the proximal diaphysis after being struck as a pedestrian by a truck. He was treated with skeletal traction for 2 months. Three years later, it was noted that he developed a valgus deformity of his left femur. An open lateral wedge osteotomy was performed to correct the valgus deformity. The second patient was a 9.5-year-old male who sustained a Gustilo grade II open left femoral fracture of the distal diaphysis after being struck by a car while he was riding a bicycle. He developed a mild genu varum deformity, which did not require surgical treatment.
Refractures
Four patients had a refracture after treatment of the open femur fracture. Three patients were initially treated with EF (1 with Gustilo grade I and 2 with Gustilo grade II fractures), and one patient was treated with traction and hip spica (Gustilo grade II fracture). From the three children treated with an EF, the first had a refracture 2 days after removal of EF (total EF duration 80 days), the second child refractured 6 days following EF removal (total EF duration 74 days) and the third refractured 1 day after removal (total EF duration 61 days). We cannot conclude that these refractures were due to early removal as mean duration of EF treatment was 71.7 days in these three cases. The average time to refracture for all four children was 3.5 months (range 3.3–4.0 months). The refractures were initially treated with a hip spica in three patients and IM nailing in one patient. The final treatment modalities for the refractures consisted of IWBB, hip spica, EF and IM nailing, respectively. The average time to healing was 9.6 months (range 7.3–14.4 months) (Table 3).
Refracture data
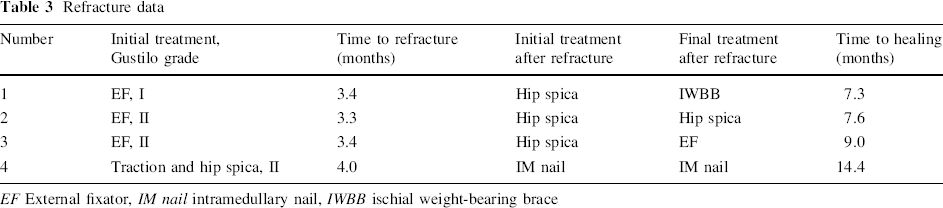
EF External fixator, IM nail intramedullary nail, IWBB ischial weight-bearing brace
Limb length discrepancy
Four patients developed a LLD of >2 cm, with an average limb length discrepancy of 3.3 cm (range 2.3–5.0 cm), and seven patients had a LLD of ≤2 cm (mean 1.2 cm, range 0.5–2.0 cm). The patient who had a 5.0-cm discrepancy also had a valgus deformity and had been originally treated with skeletal traction for 2 months and hip spica for 3 months. Following the hip spica cast, the patient underwent bone grafting to the fracture site for delayed union and was discharged with an IWBB. However, less than 1 month later, he refractured through the original callus after a fall, which was managed with an IM nail. An open wedge distal femoral osteotomy was performed to correct the valgus deformity. Seven of the patients who developed a LLD had been treated with traction and hip spica, two with IWBB, one with EF and one with ORIF.
Discussion
Open pediatric femur fractures are rare and typically occur in the older child and adolescent as a result of high-energy injuries. Associated injuries and complications are often present [2, 3, 5–7, 10]. Although numerous studies have been published on the management of closed fractures of the femur in children, a review of the literature revealed that only a few studies have been carried out on open femur fractures in this patient group [2, 7, 10, 14]. The purpose of this study was to describe the demographic and clinical characteristics of children and adolescents who presented with open femur fractures and associated injuries, and to explore associations between age, gender, type of treatment, Gustilo grade and type of wound closure, and time to union.
We report on 37 open femur fractures in 28 male and nine female pediatric patients. The mean age (11.5 years) and range (2.8–18.1 years) of the patients in our study are similar from those reported in the literature [2, 10]. The finding that 75.7% of fractures occurred in boys in our study is similar to that reported by other authors (69.8%) [2, 10] and is consistent with a higher overall incidence in males than with females. This finding is corroborated by population-based studies on childhood femur fractures [25, 26], which also identified adverse socioeconomic conditions as being significantly associated with higher rates of fracture. Most of the accidents causing the injuries in the present series (70.3%) were caused by motor vehicle accidents involving pedestrians, bicycles, motorcycles, ATVs or car crashes. The other injuries were caused by falls from a height, recreation sports, avalanche and gunshot. These mechanisms of injury are similar to those reported in other studies on open and closed fractures of the lower extremities in children [2, 7, 10, 27–29]. However, the most recent studies report greater numbers of motorcycle- and sporting-related accidents than earlier studies. A recent review on unintentional injuries in adolescents [30] identified that transportation-related injury is the largest source of these injuries (drivers, passengers, cyclists and pedestrians) and is a significant cause of disability and mortality in the 10- to 19-year-old age group. In recent years, a substantial increase has been observed in childhood ATV-related injuries [31], with a reported incidence of 22% for fractures of the lower limbs, 15% for other fractures and 14% for intracranial injuries [32]. The incidence of motorcycle-related injuries is also increasing in children and adolescents; one quarter of these accidents occurred in children <10 years of age, and most of these injuries occurred off road, outside of any legislative framework [33]. A recent Canadian study reported that all motorcycle-related injuries occurred during the summer months [34]. These findings indicate the importance of educating children, youth and their families on the importance of safer riding and the use of safety equipment in sports and leisure, as well as on the severity of the types of injuries that can arise when safety precautions are not taken [30, 35, 36]. Incentives, such as increasing parental liability, training requirements, prevention programs and media education campaigns, and stricter enforcement of existing laws should be implemented [33, 35], and these should especially target high-risk groups.
Most of the fractures in our series were Gustilo grades I and II, similar to the findings reported by Robertson et al. study [7]. A study by Hutchins and colleagues [2] had 25 grade I fractures, eight grade II fractures and ten grade III fractures. Ramseier and colleagues [10] reported nine grade I fractures and 13 each of grade II and grade III fractures, indicating a sample with more severe injuries. Associated injuries occurred in 65% of the children included in this retrospective review and seemed to occur more frequently in those with Gustilo grades I and II fractures. This high rate of associated injuries in this population indicates the importance of performing a complete physical examination in children and adolescents presenting with an open fracture of the femur to investigate the presence of other serious injuries.
In our series, traction and hip spica was used as the treatment mode in 29.7% of fractures, closely followed by EF (24.3%). Close to one fifth of patients were treated using an IM nail, followed by ORIF, and one tenth were treated using traction and IWBB. The mean age of the patients was lowest for those treated with traction and hip spica (mean 8.2 years, range 3.8–12.2 years) and highest for those treated with an IM nail (mean 15.7 years, range 13.3–17.9 years).
A previous study on 11 open femur fractures of the femur in children [7] reported that traction and hip spica were used in four patients, IM nail in three patients and immediate hip spica cast immobilization in two patients. Similar to our findings, the younger patients were treated with traction and hip spica, and the older ones with IM nail. A spica cast was also the commonest treatment method in a study on 44 open femur fractures in children [2], followed by EF, IM nail, ORIF and pins and plaster. This study found an increase in time to union with the use of EF compared with spica casts, IM nail and ORIF. However, it is difficult to ascertain whether this finding is due to the treatment type or to the severity of the injury. EF is the preferred treatment method in patients who have multiple trauma and greater soft tissue injuries. Our findings indicate an increased number of refractures and a longer time to union in children treated with an EF as compared to other treatment options. Ramseier and colleagues [10] reported a 26% rate of refractures in the EF group. Time to union was also statistically significantly longer in the EF group (16.3 weeks) compared to the IM nail (10.1 weeks). We therefore recommend removal of the EF as soon as the soft tissue problems are solved and to switch to another method of treatment to ensure prompt healing and to prevent the risk of refracture. Indeed, switching to an IM nail after the soft tissue injuries are stabilized has been suggested previously [10].
The mean union time in our series was 5.1 months, with a significantly longer time to union in grade II and III fractures than grade I fractures. Previous studies have indicated that fracture grade affects union time in open femur fractures in children [4, 7]. Our findings do not indicate a significant difference in healing time according to age. However, previous studies [2, 7] have indicated that younger patients had a shorter healing time than older patients. This may be due to the fact that our sample included several different treatment options and that other factors such as Gustilo grade, associated injuries and presence of complications also play a role on healing time. Our findings indicate a higher time to union in higher grade fractures. Contributing factors may include increased extensive soft tissue injury, higher complication rates and more associated injuries in higher grades fractures; although, these factors were not statistically explored in our study.
This study used a retrospective design; therefore, we were limited to the information which was available in the medical charts. Identifying which factors were associated with complications, such as whether an infection or delayed union occurred due to the patients’ age, Gustilo grade, fixation type or number of associated injuries, was not possible due to very small sample sizes in categorical variables (such as type of treatment and type of wound closure).
In conclusion, open fractures of the femur are rare in children and adolescents and are often accompanied by associated injuries. Several treatment options for open fractures of the femur exist, including traction and hip spica, flexible and solid IM nails, plate fixation and EF. In isolated cases of femoral fractures in children, treatment with EFs should be avoided as our data do show numerous complications with this modality (pin tract infections, delayed unions and refractures after removal of EF). Depending on the child's age, we suggest that the ideal treatment includes hip spica application in children younger than 6 years of age, flexible intramedullary nailing (FIN) in children between 6 and 12 years of age and solid IM nails in adolescents. FIN in pre-school children with femoral shaft fractures allows early mobilization and full weight bearing [37], but is not indicated in adolescents with unstable fractures [38] or in overweight or obese children [39]. In children with multiple injuries, specifically those with Gustilo grades II and III, EF still has a place as it provides immediate stability of the fractures and allows early mobilization of the child, care of the wound and ease of management of associated injuries.
Footnotes
None.