
Abstract
Purpose
Patients with lumbosacral agenesis characteristically sit on their iliac wings with their torsos bent forward, which yields an increase in intra-abdominal pressure and, subsequently, negative effects on their diaphragm. The sacrum is not available as an anchor point for instrumentation. Dunn-McCarthy rods or Galveston fixations cannot be performed due to these limited anatomic properties. On the other hand, the absence of necessary bone mass for fusion anteriorly limits the fusion interventions to the posterior. Therefore, a secure and rigid fixation is essential to preclude the need for an external support. There are limited publications discussing different techniques due to the relatively rare incidence of the disease. We report the clinical and radiological results of a new technique applied to three patients in which previously recommended methods are modified.
Methods
Two 6-year-old female patients and one 5-year-old male patient with lumbosacral agenesis underwent posterior lumbopelvic instrumentation and fusion. Together with standard pedicle screw spinal instrumentation, pelvic fixation is obtained with a combination of supero-inferior directed rod and/or screw to overcome deforming forces created at the flexion–extension pivot points of the lumbopelvic junction. Autogenic anterior tibial cortical structural graft is used for laminopelvic bridging, and demineralized bone matrix is used for the augmentation of osteoinduction. A single leg hip spica is applied for 4 months to protect the fixation.
Results
Total correction yielded an aligned spine with a posture that allows for sitting on the ischial spines for all three patients. Solid fusion was observed to maintain this correction at the final follow-up.
Conclusion
The use of new-generation pediatric spinal instrumentation systems with a new technique without knee disarticulation provides a safe and effective fixation and fusion in lumbosacral agenesis.
Introduction
Surgery has great challenges in lumbosacral agenesis due to the pathognomonic pelvic anatomy, together with the absence of a big bone segment. There are limited publications discussing different techniques due to the relatively rare incidence of the disease.
Some distal lumbar segments are absent together with the sacrum in lumbosacral agenesis; this leads to trunk shortening and sitting problems due to the hypermobile lumbopelvic junction. Iliac wings meet at the midline and are situated parallel to each other. The sacrum is not available as an anchor point for instrumentation. Dunn-McCarthy rods or Galveston fixations cannot be performed easily due to these anatomic properties. On the other hand, the absence of anterior bone mass for fusion obligates a posterior fusion procedure. Therefore, a secure and rigid fixation is necessary to maintain correction and to achieve solid fusion and preclude the need for a long-term external support [1]. We report the clinical and radiological results of a new technique applied to three patients in which previously recommended methods are modified.
Materials and methods
Two 6-year-old female patients and one 5-year-old male patient with lumbosacral agenesis were admitted to our clinic with total absence of lower lumbar vertebrae and whole sacral vertebrae. The female patients were paraplegic with severe kyphosis at the hypermobile lumbopelvic region, which forced their bodies to lean forward and made them sit on their iliac wings. The 5-year-old male patient was operated on for hip and knee flexion contractures previously. He was able to stand with external support but unable to walk. Additionally, Case 1 needed a colostomy and nephrostomy (Figs. 1, 2, 3, and 4).

Preoperative clinical pictures of Case 1 with lumbosacral agenesis. A 6-year-old female patient with typical “Buddha appearance” having severe lumbopelvic kyphosis and sits on her iliac wings. The patient has colostomies and nephrostomies
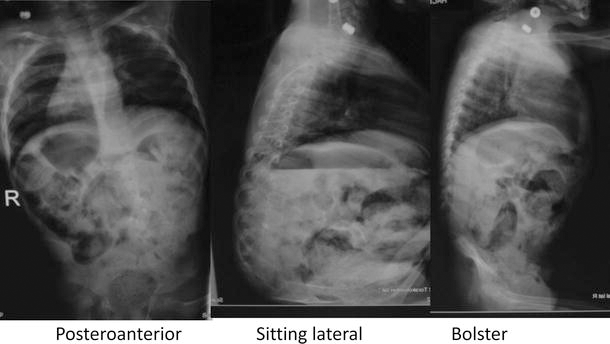
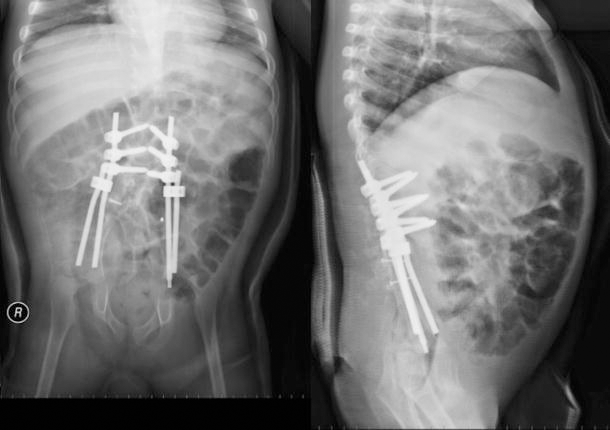
Preoperative X-rays of Case 1: posteroanterior, sitting, and bolster X-rays show the absence of sacrum and lower lumbar vertebrae. Flexible lumbopelvic kyphosis is observed. The iliac wings have lost their physiological divergent angle to each other and lie parallel and join at the midline

Intra-operative clinical pictures of Case 1: harvesting of the right anterior tibial cortex for autogenic graft and placement of an intramedullary rod for augmentation of the donor tibia

Intra-operative clinical picture of Case 1: posterior lumbopelvic instrumentation with the use of pedicle screws situated at the thoracic 12th, lumbar 1st, and lumbar 2nd vertebrae and both iliac wings connected with two rods. The autogenic tibial anterior cortex is fixed with laminar wires as a lumbopelvic bridge to enhance fusion
Together with standard pedicle screw spinal instrumentation in the thoracic 12th vertebrae, lumbar 1st and 2nd in Case 1, and thoracic 8th to 12th vertebrae in Case 2, thoracic 11th to lumbar 1 in Case 3 pelvic fixation was obtained with a combination of supero-inferior directed divergent rod and/or screw to overcome deforming forces created at the flexion–extension pivot points of the lumbopelvic junction. The autogenic tibial anterior cortex was used as a graft for fusion instead of the previously recommended total tibial autogenic graft obtained from knee disarticulation. Right tibial anterior cortexes were obtained during the index procedure in all patients. Harvested cortex was split in half horizontally and fixed to the last lamina with a sublaminar wire and to the iliac wings with a 3.5-mm cortical screw. This structural graft was used for laminopelvic bridging and autologous cancellous graft for supplementation. Demineralized bone matrix (DBM) was added for the augmentation of osteoinduction (Fig. 5). The donor tibia was secured intramedullary with a thick Steinmann pin in all patients (Fig. 6). A single leg hip spica cast was applied for 4 months. Patients were followed up clinically and radiologically for 1 (5-year-old male), 2, and 6 years (6-year-old females), respectively.
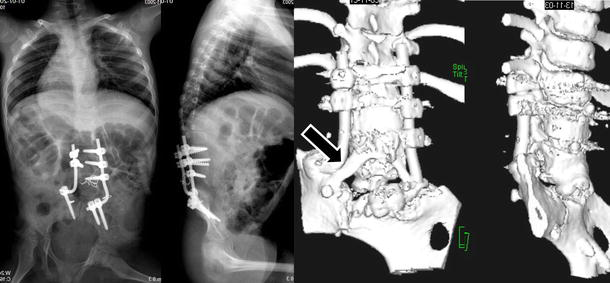
Follow-up X-rays and three-dimensional computed tomography (3D CT) scanning of Case 1: posteroanterior, lateral X-rays and 3D CT pictures show the maintenance of correction obtained at the lumbopelvic bridge and fusion at 2 years follow-up. The arrow indicates an osseous bridge formation between the lamina and iliac wing

Follow-up clinical picture of Case 1: clinical picture shows sitting posture at 2 years follow-up
Results
One-, two-, and six-year clinical and radiological follow-up of Cases 1, 2, and 3, respectively, yielded that total correction providing an aligned spine and sitting on the ischial spines are observed to be obtained in all patients and solid fusion demonstrated that this correction was maintained (Figs. 7, 8, 9, and 10). Defects at the donor tibia showed signs of bony filling at 1-year follow-up X-rays. Sitting difficulties and difficulties in transfer from chair to bed and bed to chair in all patients were successfully addressed with the surgical intervention. No significant change in hip contracture (40° approximately) was observed following surgery. The patient who was able to stand preoperatively did not lose his standing ability. No complications related to surgery were observed in any of the patients.
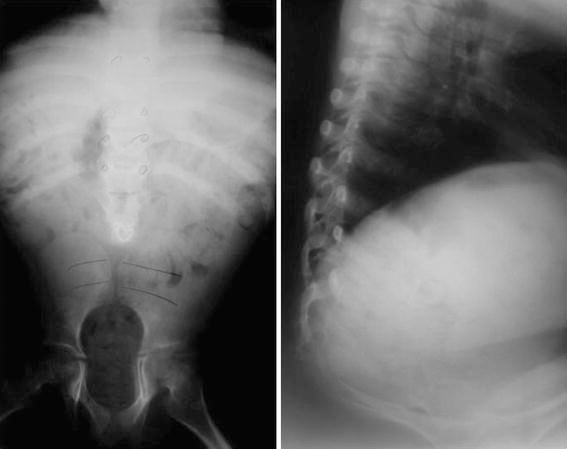
Preoperative X-rays of Case 2 with lumbosacral agenesis: lateral and posteroanterior X-rays of a 6-year-old female patient shows severe lumbopelvic kyphosis and total absence of sacrum and lower lumbar vertebrae. Both iliac wings are parallel to each other and join at the midline. The patient sits on her iliac wings

Follow-up X-rays and clinical picture of Case 2: 6-year follow-up X-rays show successful reconstruction of a well aligned lumbopelvic bridge with solid fusion by the use of thoracic 8th to 12th vertebrae to iliac wings pedicle screw-rod fixation and tibial anterior cortex autogenic grafting. The clinical pictures illustrate the patient sitting on her ischia instead of iliac wings and having a well aligned lumbopelvic region
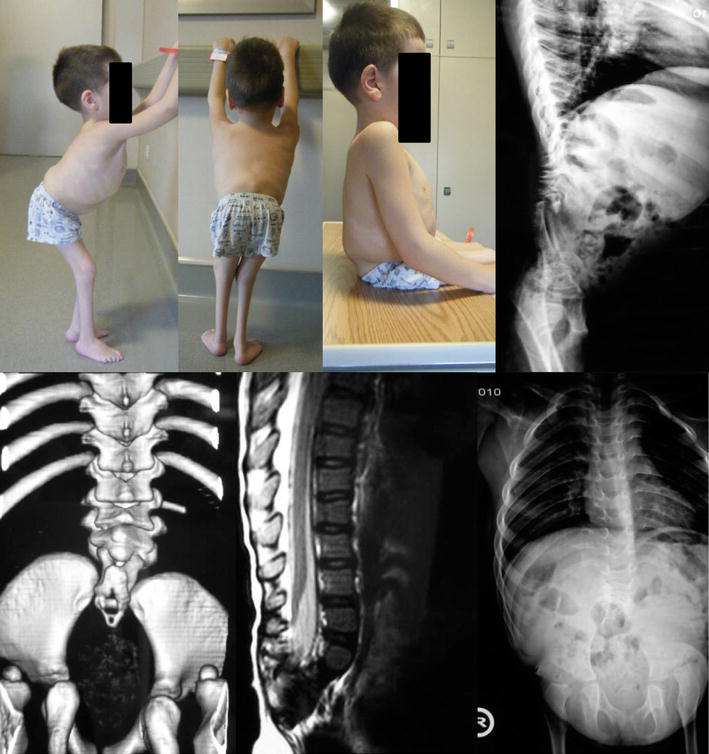
Preoperative clinical pictures, X-rays, magnetic resonance imaging, and 3D CT scans of Case 3 with lumbosacral agenesis. The clinical pictures and radiology of the 5-year-old male patient shows severe lumbopelvic kyphosis and total absence of sacrum and lower lumbar vertebrae. Both iliac wings are parallel to each other and join at the midline. The patient sits on his iliac wings and can stand by having an external support
Follow-up X-rays of Case 3: 1-year follow-up X-rays show successful reconstruction of a well aligned lumbopelvic bridge with solid fusion by the use of thoracic 8th to 12th vertebrae to iliac wings pedicle screw-rod fixation and tibial anterior cortex autogenic grafting
Discussion
Patients with lumbosacral agenesis sit on their iliac wings instead of ischial spines and their torsos are bent forward. This posture creates a characteristic spino-pelvic alignment that causes a decrease in abdominal and thoracic cage capacity. A surgical approach should yield an aligned spine over the pelvis. Instrumented correction of this deformity to create a solid fusion providing a rigid spino-pelvic bridge is the aim of this surgery.
The lack of sacral bone limits the achievement of a strong anchor site for the distal part of instrumentation as well as a bony fusion. A kyphotic, mobile lumbopelvic transition zone with minimal soft tissue covering and iliac wings situated parallel to each other (physiological divergence is lost) produce high pivotal moments. These moment forces should be overcome by strong instrumentation designs which may give rise to soft tissue problems due to the use of bulky metallic instruments. Several authors reported their results with different instrumentation systems and various graft sources in lumbosacral agenesis patients. Harrington, Cotrel-Dubousset, or Luque instrumentation systems with Galveston techniques were reported for lumbopelvic fixation in lumbosacral agenesis patients. Fusion was augmented by allogenic grafts and autogenic tibial structural grafts obtained from knee disarticulations [1–5]. Neither an iliac bolt nor sacral 1st and 2nd screws can be applied successfully to sacral agenesis patients due to the agenesis of sacral bone and the parallel orientation of both iliac wings. Jackson's intra-sacral rod or Fackler rod techniques are not suitable because of similar shortcomings. Dunn-McCarthy rods are placed at the angle between the ilium and sacrum and stabilized with ilio-sacral ligaments which are not present in lumbosacral agenesis.
We used a new-generation spinal instrumentation system in three of our patients with lumbosacral agenesis. Thoracic and lumbar pedicle screws were used for fixation at the cranial portion of the instrumentation. Pelvic fixation is achieved via a combination of a supero-inferior directed rod and/or screws placed divergent to overcome deforming forces created at the flexion–extension pivot points of the lumbopelvic junction. Left autogenic tibial anterior cortexes are used as a graft, together with allogenic DBM for fusion. All patients did well postoperatively and stayed in a single leg cast for 4 months. Well aligned axial skeleton with bony fusion over the lumbopelvic region was observed at 1 year follow-up. Patients were able to sit on their ischia.
There is a speculation about a decompensation of hip flexion contractures following spino-pelvic fusion in these patients due to the loss of spino-pelvic hypermobility that is thought to be a compensatory mechanism [6]. None of our patients suffered from an enhanced hip flexion contracture following fusion.
The use of new-generation pediatric spinal instrumentation systems using a new technique without knee disarticulation provides a safe and effective fixation and fusion in lumbosacral agenesis.