
Abstract
Purpose
To evaluate the short-term results of the non-surgical Ponseti method training programs run in Ho Chinh Minh City, Vietnam.
Methods
A questionnaire was developed and distributed to the 57 trainees who had completed one of the 3-day training courses.
Results
Of the 57 questionnaires distributed, 36 (63%) were completed and returned for evaluation. Most responders were continuing to use the Ponseti method for management of clubfoot. On average, each trainee had treated 16 babies with clubfoot, most of whom were less than 12 months of age, within 2 years of the initial training course and were achieving good clinical correction. The major problems identified were the inability to perform an Achilles tenotomy, lack of availability of the foot abduction splint, and parent compliance. The course materials were being used for reference and for dissemination of the Ponseti method to other clinical peers.
Conclusions
Evaluation of the Ponseti method training program for management of clubfoot in Vietnam revealed continued use of the technique at 12–24 months post-training. A longer term and more objective assessment of the babies/children treated and of the associated gait function and foot comfort would be beneficial.
Keywords
Background
The Ponseti method for management of infant clubfoot deformity has rapidly gained favor world-wide in the last decade. Dr. Ignacio Ponseti (1914–2009) developed and pioneered this non-surgical method in the 1940s and collated outcome records spanning 40 years which showed very good results in terms of pain and foot function in more than 95% of typical congenital clubfeet [1].
The original technique has been refined over many years, and current research continues to refine the method and its application. The implementation of the Ponseti technique has repeatedly demonstrated radical reductions in clubfoot surgical procedures and greatly improved long-term results [2]. Complications are relatively few, and cost savings are significant. In Vietnam, the cost of applying the Ponseti method is less than half that required for clubfoot surgery [3, 4] and, when correctly performed, provides better clinical results [2, 5, 6].
The developing world has been fertile ground for both the development and practice of the Ponseti method. The Uganda clubfoot project outcomes have served to inform the world of the advantages of public health policy approaches that incorporate the Ponseti method for management of clubfoot [7].
The International Committee of the Red Cross–Special Fund for the Disabled (ICRC–SFD) identified the need for formalized training in the Ponseti method in southern Vietnam and convened, in collaboration with the Vietcot Prosthetic and Orthotist School and the Rehabilitation Centre for Paraplegic Children, three seminars for doctors and physical therapists in Ho Chinh Minh City (March 2007, September 2007, May 2008) to be trained to use the Ponseti method for management of infant clubfoot deformities [4]. Between March 2007 and May 2008, a total of 271 doctors and therapists attended one of the three education seminar days, and 57 attended one of the three extended 3-day training programs aimed at teaching participants apply the Ponseti technique.
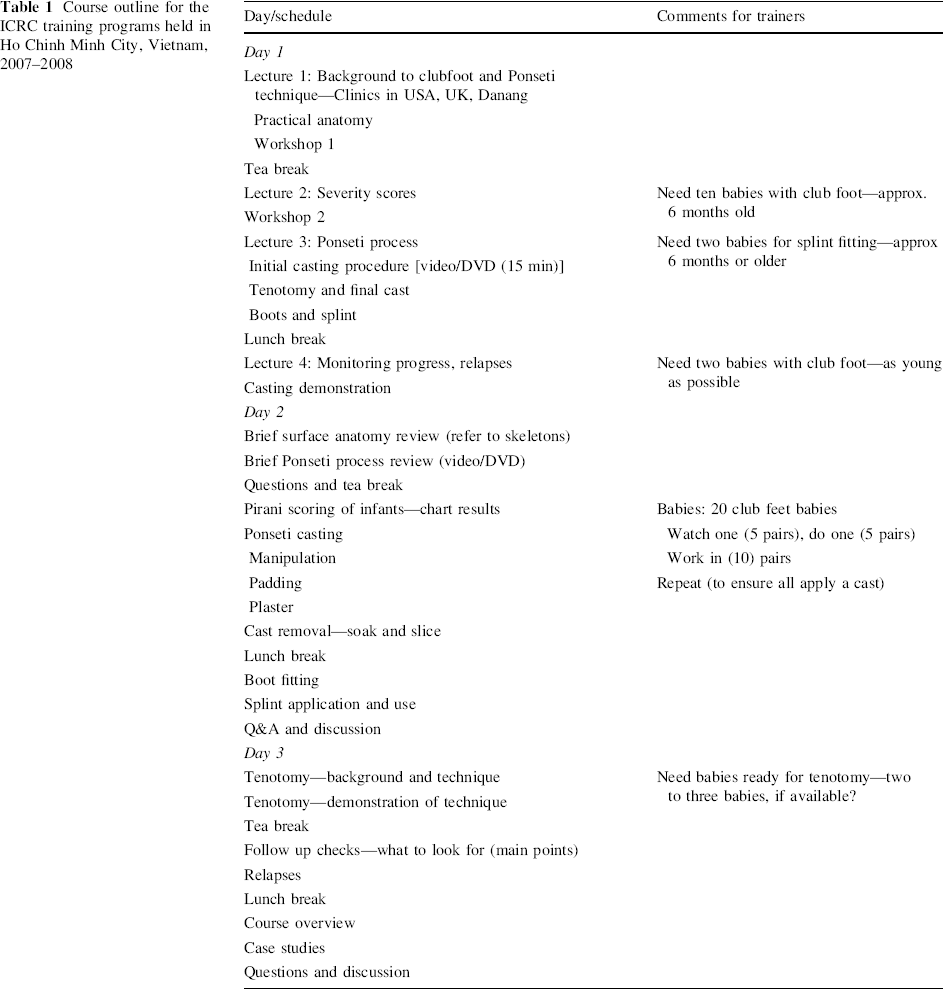
The course consisted of 4 days in total, with the first day designated a general seminar for hospital and government policy administrators, senior medical staff, and trainees. Approximately 100 attended the first day. The aim of the first day was to provide an overview of the Ponseti method for clubfoot management, including the better long-term outcomes in comparison to surgical management, cost comparisons, and a demonstration of both casting and bracing techniques. During the following 3 days, between 20 and 25 doctors and therapists were given a very structured training course in all aspects of the pediatric clubfoot assessment and management using the Ponseti method. The pedagogy was based on practical reinforcement of theory, stage-by-stage, which was important given that all oral lectures were being translated from English to Vietnamese. A basic outline of content and structure of the 3-day training course is provided in Table 1.
Course outline for the ICRC training programs held in Ho Chinh Minh City, Vietnam, 2007–2008
The trainers were two Australian podiatrists (one ex-USA), two Swiss prosthetist/orthotists, and a Vietnamese orthopedist (also the translator). The trainees were mainly doctors and therapists from both urban and rural clinical settings where pediatric clubfoot was experienced as a clinical presentation with varying frequency. Some trainees were seeing only one or two clubfoot cases each year in rural provinces, while others in large city maternity hospitals were treating approximately 500 clubfeet per year.
Aim
In common with many aid and assistance projects, the primary goals of this project have been to educate and raise awareness of the benefits of treating infant clubfoot deformity with the Ponseti method. To this end, it is necessary to build the community's capacity not only to treat but ultimately, and critically, to evaluate the results of such a program in both the short and longer term. This paper mainly addresses the short-term survey results of the ICRC-SFD training projects run in Ho Chinh Minh City, Vietnam.
Results
The results of this project need to be considered in context. Therefore, an informal report and specific local outcomes as well as the survey findings are presented here.
Anecdotal
Prior to 2006, approximately 10–12 children aged 4–10 years were presenting annually to the Centre of Paediatric Orthopaedic Rehabilitation, Ho Chinh Minh City, for revision of previous clubfoot surgery. Since 2006, this same center has been treating annually approximately 30 infants (<4 years of age) with untreated clubfoot by the Ponseti method, with the treatment provided by doctors and therapists who have attended the ICRC training sessions [3, 4].
Local data from a course trainee
Dr. Le Thi Hien Nhi from the Tu Du Maternity Hospital, Ho Chinh Minh City, completed the ICRC–SFD Ponseti method training in 2007. At the subsequent seminar in May 2008, she presented a summary of the use of the Ponseti method on 30 infants (49 clubfeet) in this hospital over a 6-month period. Of the 30 infants, 19 were male and 11 female. There were 11 unilateral clubfeet (nine right feet, two left feet) and 19 bilateral cases. Twenty cases were idiopathic clubfeet, and ten had other associated pathologies. Initial Pirani scores were <3.5 in nine feet, between 3.5 and 5.0 in 11 feet, and >5.0 in 24 feet, indicating that most of the initial presentations were of moderate and severe clubfoot deformities. Results from the Tu Du Maternity Hospital's approach to club foot management using the Ponseti method have been largely rated excellent–good [4].
Survey evaluation
In order to evaluate the ICRC–SFD courses more formally, a questionnaire was developed and distributed to the 57 trainees. The initial draft of the survey instrument was made by one of the course trainers (AE); this draft was subsequently amended and revised by both ICRC–SFD team in Ho Chinh Minh City and other course trainers (PW) before being translated from English to Vietnamese. The survey tool consists of 16 questions and invites additional comment from trainees. It covers five main areas:
Demographics (questions 1–3) Post-training use of Ponseti method (questions 4–6) Access and use of all Ponseti components (questions 7–11) Results (question 12) Difficulties (question 13–16)
The questionnaire was sent to the 57 medical professionals who had completed one of the 3-day training courses and provided a mail address. The questionnaire was initially sent in April 2009, with a reminder being sent in June, 2009. In total, 36 course trainees completed and returned the survey evaluation. The raw data were entered into a spreadsheet (Microsoft Excel) by a Vietnamese–English lingual member of the ICRC–SFD team in Ho Chinh Minh City. One of the course trainers and author (AE) then imported the data into SPSS ver. 15 (SPSS, Chicago, IL) for analysis.
The survey response rates are shown in Table 2.
Summary of the survey questionnaires and completed responses from the three training courses
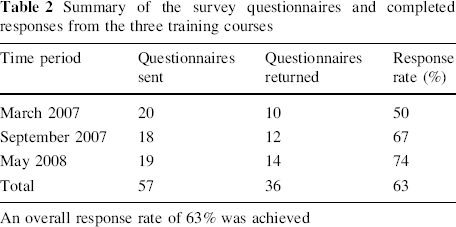
An overall response rate of 63% was achieved
The four sub-disciplines of the 36 respondents were: medical doctor (7, 19%), physical therapist (11, 31%), nurse (1, 3%), and surgeon (17, 47%).
Survey results
Of the 57 Ponseti method trainees who received a questionnaire, 36 (63%) completed and returned the survey evaluation. Of these respondents, 27 (75%) were using the Ponseti method in their workplaces. Of the nine respondents not using Ponseti method, eight reported that this was due to their not seeing any clubfoot cases.
Figure 1 shows the number of babies with clubfoot who were treated by the trainees using the Ponseti method following course attendance. A total of 465 clubfoot babies had or were being treated by 29/36 (81%) of the local doctors/therapists (January 2007–February 2009). On average, each doctor/therapist had treated 16 clubfoot babies (range 0–70).
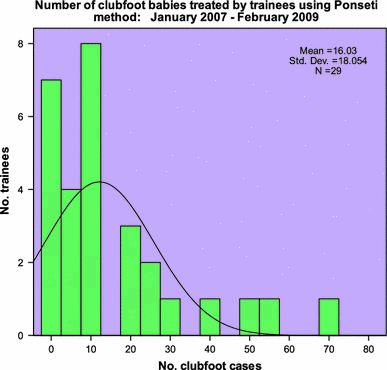
Number of babies with clubfoot who were treated by the trainees using the Ponseti method January 2007–February 2009. Based on the responses to the questionnaire, on average, each trainee had treated 16 clubfoot babies using the Ponseti method at the time of survey. The results were disparate among the trainees, with 19 treating 10 or fewer cases in the 2-year period, and three trainees treating 50 or more cases in the same period
The ages of babies treated is shown in the bar graph in Fig. 2. From the completed responses, it can be seen that in approximately half of the cases, the patient was being treated at <12 weeks of age, and 55/67 (82%) patients were treated before they were 12 months old (generally before walking ensues).
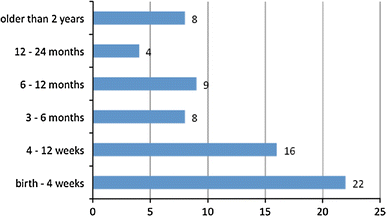
Survey responses showed that for most cases of clubfoot, application of the Ponseti method was started early in life
Of the 27 doctors/therapists using the Ponseti method following their training, 16/27 (59%) reported that the tenotomy was available to them if required. Of these, six reported that general anesthesia was used for the tenotomy procedure, nine reported local anesthesia was being used, and one reported the use of sedatives.
The foot abduction brace (FAB) was reported to be available by 23/27 (85%) Ponseti method users; four reported that the FAB was not available for their use. There were six responses which indicated that they still used the Ponseti method even though no FAB was available (implying that they used the Ponseti casting technique ± tenotomy, but no brace maintenance).
Despite the Ponseti method being presented to the trainees as a complete process (i.e., initial assessment and Pirani scoring, casting, tenotomy, FAB use, follow-up reviews), the results of this survey revealed that many trainees were using a partial Ponseti method, mainly due to either the tenotomy or the FAB being unavailable. Eleven trainees reported that they had no access to the tenotomy, although they still had treated 113 babies. A further six trainees reported no access to the FAB, and they had still treated 91 babies. One trainee reported no access to either the tenotomy or the FAB, yet had treated 12 babies (presumably with casting alone).
Twenty-five of the 27 (93%) responses indicated that the Ponseti method follow-up guidelines to monitor for clubfoot relapses were being used. (These guidelines were to follow up: 2 weeks after fitting the FAB, 3 months after fitting FAB, then every 4 months to age 3 years, every 6 months to age 5 years, every year to skeletal maturity).
Parent compliance with the application of the Ponseti method was rated by the 27 treating doctors/therapists as follows: no respondent reported 0% parent compliance; two reported 25% parent compliance; six reported 50% parent compliance; sixteen reported 75% parent compliance.
Figure 3 displays the ranked difficulties with each component of the Ponseti method as indicated by 24/27 (89%) trainees. Notable is the fact that all components of the Ponseti method are important to achieve a good long-term correction of the clubfoot deformity.
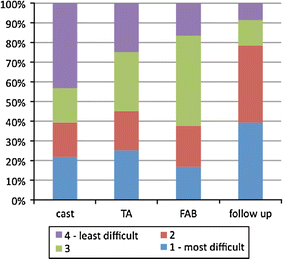
Difficulties with the Ponseti method as illustrated by the responses were: (1) initial ease of casting correction; (2) mixed availability of the tendo achilles (TA) procedure; (3) difficulty with the foot abduction brace (FAB; either compliance or availability); (4) considerable difficulty with follow-up reviews of treatment progress
Of the 27 responses received, 24 (89%) indicated that the results achieved using the Ponseti method to correct clubfoot were either excellent [8] or moderate [9]. The respondents commented on the barriers to treatment, such as distance [5], poor follow-up [5], poor parent compliance, especially with the FAB [10], no FAB available [1], and older children [3]. It was noted that the method works very well when employed early and in younger cases [11].
Twenty-nine responses were received on the use of the training course lecture notes and DVD's provided to all participants. 27/29 (93%) respondents reported using these resources and two reported that they did not.
Thirty-one of 32 (97%) responses indicated that trainees were disseminating the Ponseti technique to colleagues within their institutions. In total, these 31 responders had shared their training with 175 other colleagues (average of 8.75 per trainee). The colleagues involved were largely other doctors, physical therapists, or nurses. Twenty-five of 29 (86%) reported using the course lecture notes and DVD as a part of teaching their peers.
Thirty responses were received in relation to the need for more training. Of these, 24 (80%) indicated that they did need more training and made comments relating to which aspects of training was needed, including: follow up [1], more Ponseti, especially practical [4], anterior tibial tendon transfer [1], casting and manipulation [10], tenotomy [10], FAB [1], surgery [1], older cases [1], and updates [1].
Figure 4 shows the responses of the trainees to the parent's understanding and acceptance of the Ponseti method. The final comments reinforced these results with repeated request for “education at a grassroots” level for parents in order that they better understand and hence comply with the entire process of the Ponseti method for clubfoot correction.
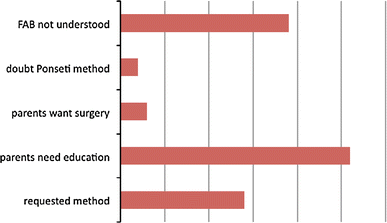
In dealing with the parents of babies undergoing clubfoot correction using the Ponseti method, the issues of not understanding the whole process and, in particular, the use of the FAB were key responses. Encouraging was the presence of parental requests for the Ponseti method, as occurs in developed countries
Discussion
The results from the ICRC–SFD training programs in Ponseti method are very encouraging. The overall response rate to the survey was 63%, thereby capturing the majority of the trainees’ responses. In essence. the evaluation of this training program in the Ponseti method for infant club foot deformity in southern Vietnam showed that most trainees have continued to use their acquired skills and knowledge of the Ponseti method in their workplaces, where it has been mostly been applied on very young infants with clubfoot. The respondents uniformly reported that they have achieved excellent to moderate results, which is in keeping with other published findings [10, 12, 13]. It is also notable that the trainees were only familiar with the Pirani scoring system, and not with a scale for incorporating a functional component, which would be relevant for a longer term survey of older children. However pleasing these results may be, they should be assessed with care as they are reported and not objectively confirmed results. It was gratifying to realize that the trainees are not only using the Ponseti method themselves, but also actively disseminating their skills and knowledge to colleagues, such that, on average, each trainee reported treating some 16 babies and training eight colleagues. Thus, it seems hopeful that the use of the Ponseti method will remain in use for the management of clubfoot deformity in babies born in Ho Chi Minh City and southern Vietnam provinces.
This evaluation has been valuable in highlighting a number of consistent problems and barriers to better clinical results using the Ponseti method. The availability of the Achilles tenotomy and the FAB were not universal, which has clear and negative implications for treatment outcomes. [The FAB (boots of nine sizes and adjustable width bars) which was used within the training courses was readily available as a complete kit from the DaNang Centre orthotics department]. It is well documented that most cases of clubfoot managed with the Ponseti method will require a tenotomy, and there is a consistent correlation between poor or inadequate use of the FAB and clubfoot relapse [8, 9, 11, 14]. In part, the ready availability of the Achilles tenotomy may be due to the trainers differing experiences with performing the simple percutaneous tenotomy using local anesthesia, in an aseptic, but clinical setting (as opposed to general anesthesia in an operating theater, making the procedure more daunting, expensive. and less accessible).
The trainees varied in terms of their prior experience with casting and knowledge of clubfoot anatomy and the complete Ponseti method. Between trainee disciplines, such as surgeons versus physical therapists, no uniform trends were observed regarding casting familiarity or use. In some clinics, the physical therapist would cast, in others the doctor or surgeon would cast. However, the trainers were able to quickly recognize those trainees who were casting regularly as they adapted more readily to the nuance of the Ponseti method casting.
The survey findings reveal an ongoing need for the education of parents as they embark upon the Ponseti method treatment course; problems were reported with follow up and the distances to travel for review. These findings are similar to those reported in other developing countries where the Ponseti method has been introduced and challenge the Western “patient attends the doctor” model of access to care [13, 15]. The repeated comments from the trainees surveyed emphasizes the need for “education at a grassroots level” for parents to understand and participate in the lengthy Ponseti method. This seems to be essential if relapses due to incomplete treatment courses are to be reduced.
There were a number of possible confounding factors with this evaluation survey. Firstly, the questionnaire itself was developed conveniently and pragmatically rather than methodically. As a result, it cannot be seen as a reliable nor necessarily valid instrument of measure. While due care was taken, there were multiple translations involved in the evaluation process: from the original English language draft to the distributed Vietnamese language version; from the Vietnamese language completed surveys to English language data entry and analysis.
Conclusion
This limited evaluation of the ICRC–SFD training program to implement the Ponseti method for management of infant clubfoot deformity in south Vietnam revealed a good uptake and continued use of the technique at 12 or more months post-training. The longer term effectiveness of this program will be indicated when/if reduction in clubfoot surgical procedures continues, as is tentatively reported. A more objective and future stage assessment of the clubfeet corrected via the Ponseti method and the associated gait function and foot comfort would be beneficial.
Footnotes
Acknowledgments
The author wishes to acknowledge all members of the Ponseti method training team: Leo Gasser and Miguel Fernandos, International Committee of Red Cross, Ho Chinh Minh City, Vietnam; Do Van Thanh and Karin Eberle, Da Nang Orthopedic and Rehabilitation Centre, Da Nang City, Vietnam; Paul Wade, Australasian College of Surgical Podiatrists, Adelaide, Australia.
Course training materials and the questionnaire are available upon request.
The author declares there are no conflicts of interest and agrees to the journal reviewing primary data if requested.