
Abstract
Purpose
Patients with neuro-orthopaedic disorders often develop hip flexion contractures or rotational hip deformities. Increasing deformities impair the already diminished walking abilities and proximal femoral osteotomies are often performed to maintain/improve walking abilities. Fixation of the osteotomies with condylar plates has been successfully used but does often not allow immediate postoperative full weight bearing. To avoid a substantial postoperative rehabilitation deficit and additional bone loss due to inactivity, a postoperative treatment with full weight bearing is, therefore, wishful. Newer fixed-angled implants with stronger anchoring in osteopenic bone might fit these demands. The objective of this study was to evaluate bone healing and the complication rate after proximal extending and/or derotational femoral osteotomy fixed with 3.5/4.5 Locking Compression Plate (LCP; Synthes®) and postoperative full weight bearing in ambulatory neuro-orthopaedic patients.
Methods
Fifteen ambulatory neuro-orthopaedic patients (12 cerebral palsy [CP], 1 trisomy 21, 2 hemiparesis) with a mean age of 13.7 years (range 7–22) with hip flexion contractures and/or rotational deformities underwent subtrochanteric (n = 26) osteotomy between July 2004 and October 2007. All patients were allowed to bear their full weight postoperatively. We investigated the fusion rate, implant failure, and general complication rate until union had occurred.
Results
Fourteen patients (mean weight 42.0 kg [range 21.8–59]) uneventfully achieved solid fusion. One patient (19 years of age, 73 kg) needed revision surgery due to implant failure with consecutive varus deformity and achieved solid fusion after the second intervention. Besides one superficial wound infection, no other complications occurred.
Conclusions
Subtrochanteric extending and/or derotational osteotomies fixed with an LCP are a reliable procedure in neuro-orthopaedic patients. Most patients can be treated with early postoperative full weight bearing. However, in heavier patients, possible implant failure must be considered.
Keywords
Introduction
Patients with neuro-orthopaedic disorders often develop hip flexion contractures or rotational hip deformities [1–3]. Increasing deformities further impair the already diminished walking abilities of these patients. Conservative treatment alone may be sufficient in the first years of life, but there is little evidence of its efficacy to maintain mobility so far [4]. Therefore, surgical procedures are being performed frequently. Whereas for flexion contractures soft tissue procedures may at least temporarily be sufficient, they hardly ever lead to longstanding satisfactory results in rotational deformities [5]. Femoral osteotomies are, therefore, done to correct the deformities. Inter- and subtrochanteric as well as supracondylar osteotomies have been described to address deformities of the femur [6, 7]. Bone quality is often diminished even in ambulatory children with neurologic disorders such as cerebral palsy (CP) [8, 9], myelomeningocele [10], or trisomy 21 [11]. Consequently, implant stability is decreased, sometimes prohibiting early postoperative full weight bearing. Additionally, many of these patients hardly reliably manage partial weight bearing due to coordinative problems and/or lacking in strength. This may necessitate a postoperative period of bed rest or wheelchair mobilization or even the application of spica casts until bony fusion occurs [6, 7]. This in turn leads to a substantial rehabilitation deficit and additional bone loss due to inactivity. A postoperative treatment with full weight bearing and as little restriction of physical activity as possible is, therefore, wishful. Recently, it has been shown that early weight bearing shows several benefits on functional recovery of ambulatory children with CP after bilateral proximal femoral osteotomies for excessive internal hip rotation fixed with blade plates [12]. We hypothesized that newer fixed-angled implants with stronger anchoring in osteopenic bone might allow for a stable fixation of proximal femoral osteotomies and early weight bearing as well.
Against that background, the objective of this retrospective study was to evaluate bone healing and the complication rate after the fixation of proximal femoral osteotomies with 3.5 or 4.5/5.0 Locking Compression Plate (LCP; Synthes®, Oberdorf, Switzerland) and early postoperative full weight bearing in a neuro-orthopaedic population.
Materials and methods
The inclusion criteria for this retrospective study were as follows: (1) ambulatory patient with neuro-orthopaedic disorder; (2) operation between July 2004 and October 2007; (3) corrective surgery for hip flexion contracture and/or rotational deformity; (4) subtrochanteric femoral osteotomy fixed with a 3.5 or 4.5/5.0 Locking Compression Plate (LCP, Synthes®, Oberdorf, Switzerland); (5) full weight bearing immediately postoperatively. Twenty-three ambulatory neuro-orthopaedic patients were operated for hip disorders in the above mentioned time period. Eight patients with 13 proximal femoral osteotomies were excluded due to simultaneous distal femoral osteotomies (n = 1) or concomitant surgical procedures that prohibited postoperative full weight bearing (n = 7). Fifteen patients with an average age at surgery of 13.7 years (range 7–22 years) fulfilled all inclusion criteria and were enrolled in the study (Table 1). Twelve patients suffered from CP, one from trisomy 21, and two from other unspecified neurological disorders with concomitant spastic hemiplegia/-paresis. A total of 26 proximal osteotomies were performed. Eight patients had unilateral and seven patients had single-stage bilateral procedures.
Details of the study population
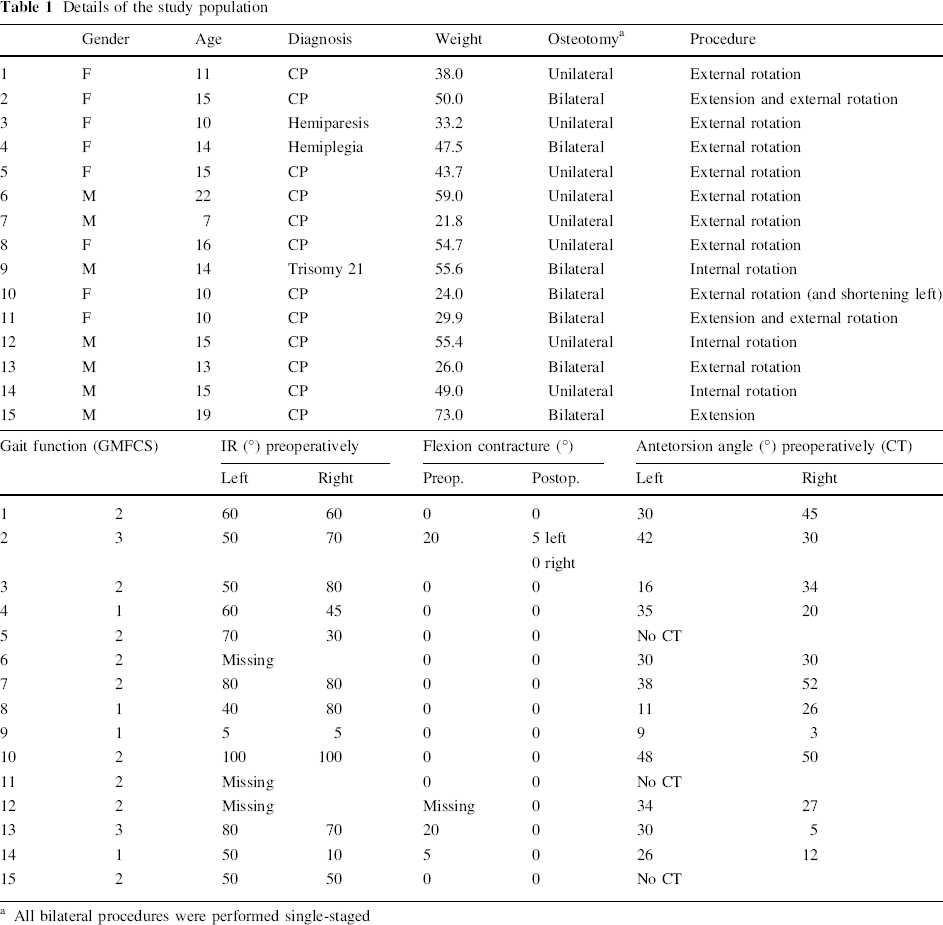
All bilateral procedures were performed single-staged
All patients underwent clinical examination of gait and lower extremity motor function in our outpatient clinics prior to the operation. Gait function was classified according to the Gross Motor Function Classification System (GMFCS; Table 1) [13]. Hip range of motion (ROM) was measured clinically with special regard to hip internal rotation and flexion contractures of the hips. Six patients had an additional extensive gait analysis done preoperatively. Postoperative gait analysis was done in three of these six patients. Preoperative computed tomography (CT) scans to determine femoral antetorsion was done in 11 patients.
All patients underwent a subvastus approach. Depending on the patient's weight and habitus, a 3.5 or 4.5/5.0 LCP was precontoured to the femoral shape. Two 2.5-mm K-wires to control rotation were placed prior to the osteotomy, which was done with an oscillating saw. After reduction of the fragments in the desired position, they were fixed with the LCP and at least two fixed-angled bicortical screws in each fragment. Plates were always put on laterally, also in extension osteotomies. In 12 osteotomies, the fragments were compressed using a standard cortical screw as a dynamic compression screw in one of the plate's combi holes. Standard wound closure without suction drainage completed the procedure.
All patients were mobilized with full weight bearing within 1 week after the operation. When possible, patients were given crutches as support without restricting weight bearing. No attempt was done to assess how much weight bearing actually took place. Physiotherapy was started on the first postoperative day, with the main focus on maintaining the surgically achieved correction of contractures and gait education. Patients were dismissed when they were able to securely climb and descend stairs and the wounds were inconspicuous. Physiotherapy was continued after dismission in all patients.
Retrospective analysis included chart review with an assessment of complications (wound healing, infection, and hematoma) and radiological workup. Solid bony fusion on plane radiographs was defined as bridging callus in at least three cortices. When only two cortices were clearly visible due to the plate being superimposed, both had to show a bridging callus. This is in line with the definition of solid bony fusion in studies of intramedullary nailing for tibial fractures, where fusion was defined to be solid when a bridging callus was seen in two [14] or three [15] of four cortices, respectively.
Results
Of 26 osteotomies in 15 patients, 24 in 14 patients (mean age 13.3 years [range 5–22], mean weight 42.0 kg [range 21.8–59]) healed uneventfully and without secondary dislocation. Eleven patients were seen for the first follow-up after 5–7 weeks, one osteotomy being fused at this time, while all others showed the beginning of fusion. Of the latter, all but two were radiographically reassessed in the second follow-up after an average of 39.9 weeks (range 11–138 weeks) and they all showed solid bony fusion. The remaining two osteotomies in one patient were not X-rayed because she was able to walk without any pain and, therefore, a solid fusion was assumed to have occurred. One patient was only seen after 10 weeks, with both osteotomies being fused at that time. The patient with trisomy 21 developed a superficial wound infection on one side, which could be managed without surgery. No other complications occurred in these 14 patients and, radiologically, no loss of correction occurred.
One 19-year-old patient with a body weight of 73 kg who underwent proximal femoral osteotomies for the correction of a flexion contracture of 15° on both sides presented with increasing pain 2 weeks postoperatively. The radiographs revealed an implant failure with varus deformity of both proximal osteotomies (Fig. 2). Fixation had been performed with a standard 6-hole 4.5/5.0 LCP with two bicortical fixed-angled screws proximally and three distally, and the patient was mobilized with full weight bearing using two crutches after 1 week. Revision surgery was performed 16 days after the initial operation and consisted of plate and screw removal and reosteosynthesis with a broad 4.5/5.0 8-hole LCP fixed with two bicortical fixed-angled screws proximally and three distally. Additionally, the two fragments were compressed using a standard cortical screw as a dynamic compression screw. After the reoperation, the patient was only mobilized in the wheelchair for 4 weeks before full weight bearing was allowed after the radiographs revealed the beginning of consolidation. The further healing process was then uneventful and radiographs taken 21 weeks after revision surgery showed a solid fusion of both osteotomies without loss of correction.
Discussion
When treating patients with neuro-orthopaedic disorders, one is often confronted with progressing joint contractures and deformities that impair gait and mobility, despite continuous physiotherapy, the use of customized orthoses, and even Botox injections. Besides luxated or subluxated hip joints, therapy-resistant rotatory femoral deformities and flexion contractures of the hip and knee are the main reasons to perform corrective surgery in this population. Most surgical procedures at the proximal femur consist of inter-/subtrochanteric corrective osteotomies that are fixed with angled plates or hip screws and postoperative treatment often includes bed rest and/or cast immobilization for some time [6, 7]. Plate or screw fixation of proximal osteotomies may also be treated without a cast postoperatively and even with early weight bearing [12, 16, 17]. A recent investigation has reported postoperative bone loss after at least 4 weeks of either non-weight bearing or casting to be as high as 34% in otherwise healthy children [18]. Whereas this may be irrelevant in a healthy child, it is of importance in a chronically ill patient with an already diminished bone density, as in CP [8, 9], myelomeningocele [10], or trisomy 21 [11]. In such a child, it may attribute to a significantly higher risk of a fracture [19–21]. The loss of strength associated with such a period of non-weight bearing leads to a substantial rehabilitation deficit in a patient who already has limited rehabilitation potential. It is, therefore, of utmost importance to get these patients walking again as soon as possible and full weight bearing immediately postoperatively would be wishful, as many will hardly manage to ambulate with partial weight bearing reliably due to lacking in strength and coordinative problems. Although the blade plate allows for reliable fixation and early weight bearing, the surgical procedure is demanding and soft tissue irritation by the somewhat bulky implant is quite frequent. We, therefore, started to use a fixed-angled plate system to fix subtrochanteric corrective osteotomies, allowing early weight bearing too. A recent study focused on subtrochanteric rotational osteotomies in a paediatric population with reduced femoral antetorsion. Osteotomies were fixed in the same way and with the same implant as in our study group, and full weight bearing was allowed immediately postoperatively. It was found that correction could be accomplished reliably and that early weight bearing with crutches was possible, even in bilateral procedures without implant failure [22]. However, besides reduced femoral antetorsion, these children were healthy without any evidence of reduced bone quality, as to be expected in our group.
In the locking plate, the force is transmitted from the bone to the plate and vice versa by the screws which are angle-stable fixed in the plate. This force transmission is not dependent on direct friction between the plate body and the bone, which has the advantage of less compromising blood supply to the bone. In vitro, a fixed-angled implant such as the LCP (Synthes®) was found to provide better resistance against axial loading in osteoporotic bone than a standard Low Contact Dynamic Compression Plate [23]. This indicates that the use of a fixed-angled implant might allow for early full weight bearing in osteopenic bone. Biomechanical investigations suggested that the fixation with at least two bicortical angle-stable screws per segment should generally be sufficient in osteosynthesis of the lower leg [24]. Based on this, we chose to use the LCP system with at least two screws in each fragment for the fixation of the subtrochanteric corrective osteotomies. The proximal was always fixed with only two screws, allowing for an as proximal osteotomy as possible. With newer angle-stable implants that are now available such as the LCP paediatric hip plate, an even more proximal osteotomy is possible, allowing for a correction as close as possible to the deformity. The surgical procedure using the LCP is technically much easier than using an angled plate. As angle stability of the screws is mandatory for secure full weight bearing postoperatively, plates have to be bent with the available screw place-holders that avoid a distortion of the threaded hole. To control rotation, the use of K-wires of at least 2.5 mm have proved to be of value because they usually resist deformation by the soft tissues. The complication rate was low, with one superficial wound infection not related to the implant. None of the patients complained about soft tissue irritation by the plate.
For most cases, the described treatment protocol lead to an uneventful bony healing of the osteotomy without loss of correction (Fig. 1). One patient, however, developed implant failure with increasing varus deformity through the osteotomy (Fig. 2a). He differed from the other patients due to his older age and higher weight, both being well above the mean of the whole study population. In his case, we initially used a standard 4.5/5.0 6-hole LCP for fixation. During revision surgery, we changed to the broad 4.5/5.0 LCP with displaced screw holes. Postoperatively, he was kept non-ambulatory for 4 weeks, after which he was mobilized with full weight bearing. Healing of the osteotomies was then achieved uneventfully (Fig. 2b). This one case probably demonstrates the limits of the described procedure with full weight bearing immediately postoperatively. In adult patients, possible implant failure must be considered and a period of non or only partial weight bearing where possible seems to be advisable.

A 15-year-old cerebral palsy (CP) patient with rotational deformity 6 weeks after subtrochanteric osteotomy showing bridging callus formation in three cortices
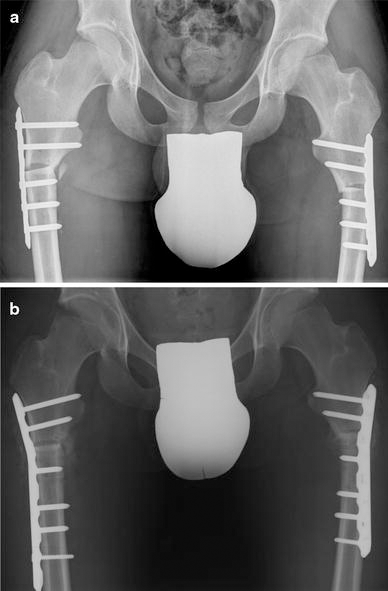
A 19-year-old CP patient with rotational deformity.
The main drawbacks of our study are the retrospective non-comparative design, the small number of patients, and the fact that follow-up controls were not after standardized time-spans. This did not allow for a more exact determination of the time point of bony fusion. However, with the exception of one case, no postoperative periods of non-weight bearing and no revision surgeries were necessary to achieve bony union. We, therefore, conclude that, in a paediatric neuro-orthopaedic population, the fixation of proximal femoral osteotomies for flexion or rotational deformities with an LCP is a safe procedure, allowing for postoperative full weight bearing, even in patients with diminished bone quality.
Footnotes
Acknowledgements
No funding has been received for this work. There are no financial conflicts of interest between any of the authors and the nature of this work.