
Abstract
Purpose
The use of 2-octylcyanoacrylate (OCA) has been evaluated for the treatment of nail bed injuries in adults. We propose to validate this technique in a continuous paediatric population of 30 children.
Methods
Patients with nail bed injuries associated with displaced fractures of the distal phalanx were excluded from the study. However, parcellar fractures of the tuft were included. After removal of the nail, wound detersion and anatomic positioning of the nail bed was done and maintained under the nail plate using a single dose of OCA. Follow-up evaluation was done at day 7 and 1 and 3 months.
Results
The mean delay between the trauma and the surgery was 13.5 h. The nail bed lesion was a single transversal wound in 27 cases. A pulpar wound was associated in 22 cases. At 3 months control (final follow-up), no pain or functional impairment was noted. The cosmetic result was excellent for the patient and his family in 30 out of 31 cases. It was excellent for the surgeon in 25 cases and good in six cases.
Conclusions
In the OCA technique, meticulous primary detersion and exact anatomic positioning of the damaged nail bed is mandatory before applying the cyanoacrylate adhesive. In our experience, we found that the OCA technique provided a fast and safe result in nail bed lesions. The final cosmetic appearance, function and patient satisfaction were good in our series. In these lesions, discomfort and inconvenience associated with suture removal could be avoided by the use of OCA.
Introduction
Fingertip injuries, especially those affecting the nail bed, are among the most common traumatic conditions presenting to paediatric surgeons and paediatric emergency departments [1, 2]. Removal of the nail plate and meticulous repair of nail bed lacerations with replacement of the nail has been shown to prevent long-term cosmetic and functional disability [3–5]. The 2-octylcyanoacrylate (OCA) group of tissue adhesives has been used extensively in both traumatic and surgical wound closures [6–15]. To date, the use of OCA, more commonly known as Dermabond (Dermabond®; Ethicon, Inc., Somerville, NJ, USA) has been evaluated for the treatment of nail bed injuries in adults [13–15]. We propose to validate this technique in a paediatric population to repair nail bed lesions. The rate of healing, cosmetic appearance and functional results were prospectively evaluated in a continuous series of 30 patients.
Materials and methods
Thirty consecutive children with acute nail bed lacerations presenting within 8 h of injury were prospectively enrolled in the study. Institutional Review Board approval and informed consent for participation were obtained. Inclusion criteria included patients with a nail plate avulsion injury with associated nail bed laceration. Patients with nail bed injuries associated with displaced fractures of the distal phalanx were excluded from the study. However, parcellar fractures of the tuft were included. At presentation, each patient's demographic information, including age, past medical history, hand dominance (for children more than 2 years old) and mechanism of injury, was recorded.
Physical examination was performed under general anaesthesia and pneumatic tourniquet. Each patient received a single dose of intravenous cefazolin. Laceration characteristics, as well as the time required to perform the nail bed repair, were documented. The treatment time was defined as the total elapsed time from the moment the tourniquet was applied to the time the dressing was finished. Nail bed repair was performed using OCA (Dermabond®). After removal of the nail (Fig. 1) and wound detersion, nail laceration was anatomically positioned and fixed under the nail plate using a single dose of OCA (Fig. 2). A non-adherent sterile dressing was then applied until day 7. Follow-up evaluation included a wound check at day 7 after repair and examinations at 1 and 3 months. At each follow-up visit, the patient-perceived functional outcome, cosmetic outcome and level of pain were assessed using three separate ten-point analogue scales, as previously reported in adults [15]. On the ten-point functional outcome scale, scores ranged from 0, which indicated complete loss of affected digit function during activities of daily living and recreational activities, to a score of 10, which indicated no functional limitation, with the patient using the affected digit without difficulty. At final follow-up, the cosmetic result (Fig. 3) was evaluated using the scale published by Zook [16].
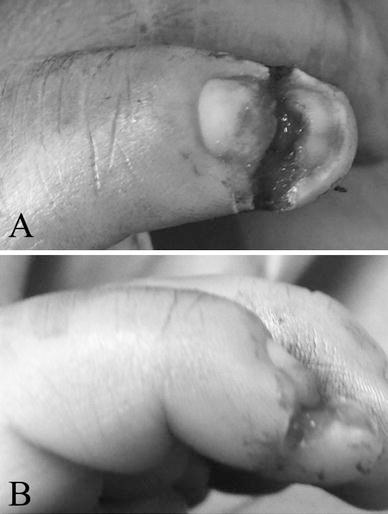
After removal of the nail, careful wound detersion was done under general anaesthesia and pneumatic tourniquet.
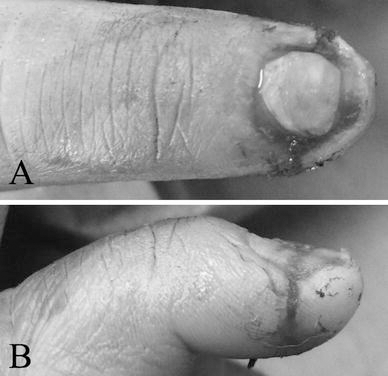
Nail laceration was anatomically positioned and fixed under the nail plate using a single dose of 2-octylcyanoacrylate (OCA).

Final cosmetic result was noted after 3 months.
Results
From November 2008 to February 2009, 30 patients were consecutively and prospectively included. One child sustained injury to two fingers. The age of the cases ranged between 8 months and 9 years (mean 2.9 years). The male to female ratio was 21:9. The majority of injuries occurred at home, the child having caught the digit(s) in a door. The mean delay between the trauma and the surgery was 13.5 h.
The nail bed lesion was a single transversal wound in 27 cases and a comminutive laceration in four cases. The nail table was avulsed but intact in 26 cases and incomplete or absent in five cases. A pulpar wound was associated in 22 cases and a parcellar fracture of the tuft was noted in ten cases. The mean operative time was 7.7 min. No adverse effects were noted during the surgery. In patients with incomplete or absent nail table, nail table replacement was done using a silastic plate. At day 7 control, no infectious complication was noted. Wound dressing was performed without any technical difficulties. Pain was absent in 16 cases and moderate in 15 cases. At 1 month control, pain was absent in 30 out of 31 cases. Functional evaluation showed a complete recovery of function in all of the cases. The cosmetic result was satisfactory for the patient and his family in 22 cases. It was very good for the surgeon in 13 cases, good in eight cases, mild in eight cases and fair in two cases.
At 3 months control (final follow-up), no pain or functional impairment was noted. The cosmetic result was excellent for the patient and his family in 30 out of 31 cases. It was excellent for the surgeon in 25 cases and good in six cases.
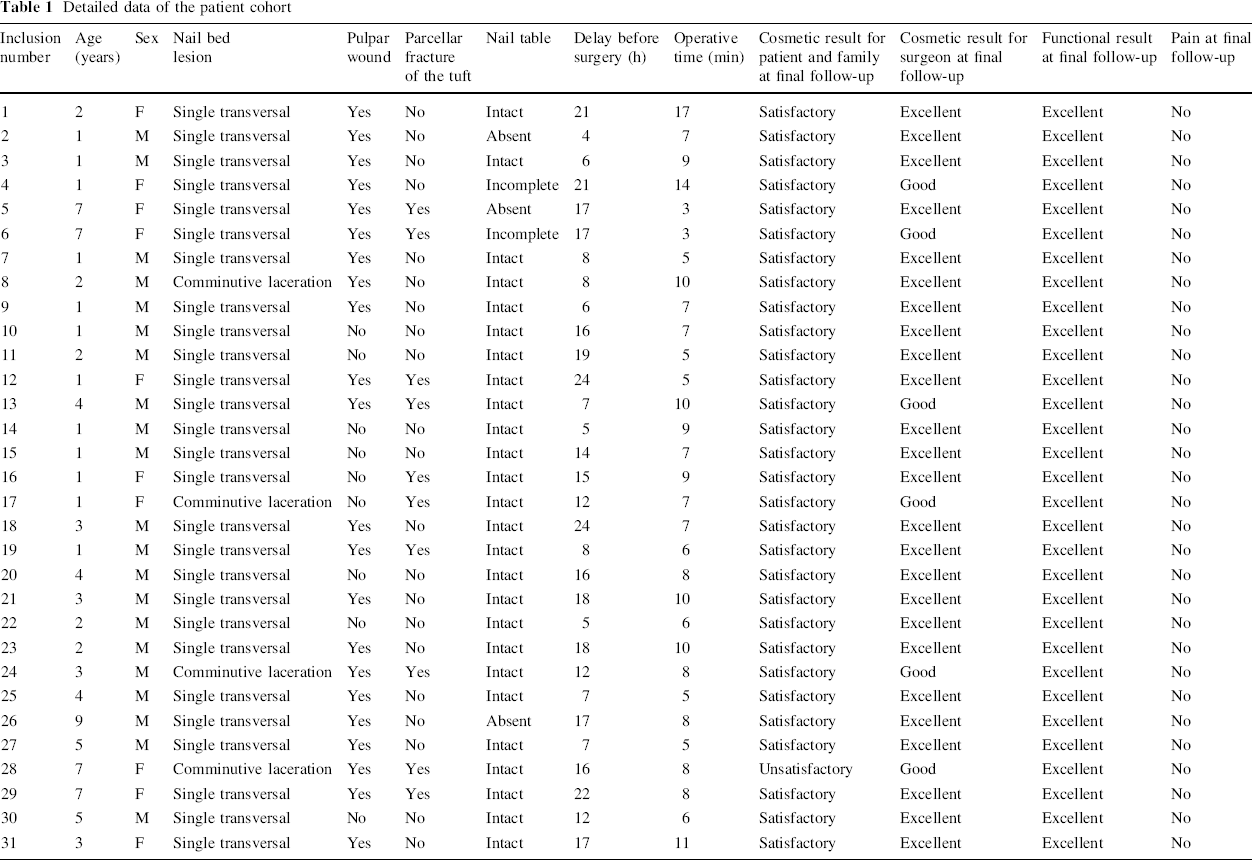
The clinical data are presented in Table 1.
Detailed data of the patient cohort
Discussion
Conservative treatment has been accepted as a method of treatment for all fingertip injuries in children, including the nail bed, because of its simplicity and low cost [4]. However, a high incidence of post-traumatic nail deformity and frequent poor results following secondary repair have been reported [17, 18]. Some studies [18, 19] showed a benefit of careful assessment and meticulous repair of injuries to the nail bed. Following surgery, good results can be expected, deformities and morbidity are prevented and the need for further surgery is avoided [4]. Conventional suture repair using magnification was practised in our department for many years with satisfactory results. In the paediatric population, accurate surgery frequently demands general anaesthesia, which is safe in the appropriate circumstances [20, 21]. In our series, there were no anaesthetic complications.
Since cyanoacrylate adhesive or ‘superglue’ was first introduced, it has been refined to 2-butylcyanoacrylate and, more recently, to OCA [22], with improvement in its strength and flexibility [23]. Animal studies have confirmed that cyanoacrylate adhesive does not interfere with wound healing [24], has minimal toxicity [25] and may reduce the incidence of wound infection [26–28]. The United States Food and Drug Administration (FDA) has granted approval for its use in humans. The potential advantages of tissue adhesive include ease of use, painless application, rapid closure, cosmesis, avoidance of needlestick injuries and removal of the suture or staples [10]. OCA is now widely used for wound closure [8–10]. The use of tissue adhesives has been described in orthopaedic surgery [22] but, especially in children, the most common skin closure remains to be staples or subcuticular suture.
In the OCA technique, meticulous primary detersion and repair with removal of the nail in order to expose the damage to the sterile and germinal matrix has been the rule. Exact anatomic positioning of the damaged nail bed is mandatory before applying the cyanoacrylate adhesive. Diaphyseal fracture of the distal phalanx impairing fingertip stability and nail bed lesion was not compatible with this technique. In such cases, percutaneous wiring of the underlying fracture associated with nail bed suture and nail table repositioning were performed.
In our experience, we found that nail bed repair performed using OCA was faster than suture repair, while providing similar cosmetic and functional results. The final cosmetic appearance, function and patient satisfaction were good in our series. In these lesions, discomfort and inconvenience associated with suture removal could be avoided by the use of OCA. In older and cooperative children, this technique could be performed in the emergency department under conscious sedation, which would result in cost savings. Nevertheless, we currently perform this technique under general anaesthesia.
Some of the possible limitations to this study are that the advantages and inconveniences when using OCA were not compared with another control group with conventional suture repair. However, these two techniques were already compared in adults, showing similar results in both groups [15]. Long-term cosmetic results need to be evaluated in our cohort. However, the early results with a 3 months follow-up were satisfactory in most of the cases.
In our experience, repair using OCA (Dermabond®) is a safe technique for the treatment of nail bed injuries in children. This technique is currently used in our department.