
Abstract
Abstract
Purpose
Residual midfoot and hindfoot deformities in rigidly deformed feet present a very complicated surgical dilemma. A plantigrade foot is desirous for proper lower extremity mechanics in a child with ambulatory potential. In this group of patients, soft tissue procedures are no longer an appropriate option, and well-recognized hindfoot procedures, such as talectomy, have many disadvantages. This study reviews the results obtained using multiplanar supramalleolar osteotomy as a salvage procedure to correct deformities of the complex rigid foot in children.
Methods
A retrospective review was conducted of 27 multiplanar supramalleolar osteotomies in 18 children. The underlying diagnosis of the patients included seven severely rigid idiopathic clubfeet, five arthrogryposis, two myelodysplasia, one Ellis-van Creveld, one Streeter's, one cerebral palsy, and one severe burn contracture. The average age at surgery was 5.6 years, and follow-up averaged 8 years. A successful outcome was deemed a plantigrade foot on physical exam with follow-up of at least 2 years and no subsequent tibial surgeries. All failures were included regardless of the length of follow-up.
Results
A plantigrade attitude of the hindfoot was obtainable at the time of surgery in all cases. Eighteen of the 27 feet had a successful outcome. Nine of 27 (33%) feet had recurrence of the foot deformity requiring additional surgery. Time to recurrence averaged 5.7 years (9 months–13 years). Complications from the surgery included four minor wound healing problems, two delayed unions, and one screw recession, all of which healed without consequences. There was no evidence of nonunion, growth plate closure, infection, or fracture above or through screw holes.
Conclusion
The multiplanar supramalleolar osteotomy appears to be a reasonable salvage procedure for severely scarred and complex rigid foot deformities and can be reinstituted for failures due to remaining growth.
Introduction
Residual foot deformities in complex rigid feet present a difficult surgical dilemma for the treating physician. In the context of this paper, the complex foot is defined as one with a rigid, inflexible deformity on clinical exam; has undergone at least one or more attempts at surgical correction of the deformity; or has a severe, intrinsic abnormality that renders the foot prone to inevitable further deformity (Figs. 1, 2). The inherent rigidity of the foot makes manipulation, orthotics, or soft tissue procedures no longer feasible as an option for correction. Well-recognized foot procedures such as talectomy have many shortcomings in what are usually smaller, immature feet. Disadvantages include shortening an already small foot, additional diminished motion, and commonly encountered osseous immaturity of the foot. Supramalleolar osteotomy has been described as a reasonable alternative to these procedures in the management of residual equinus deformity in older children [1].
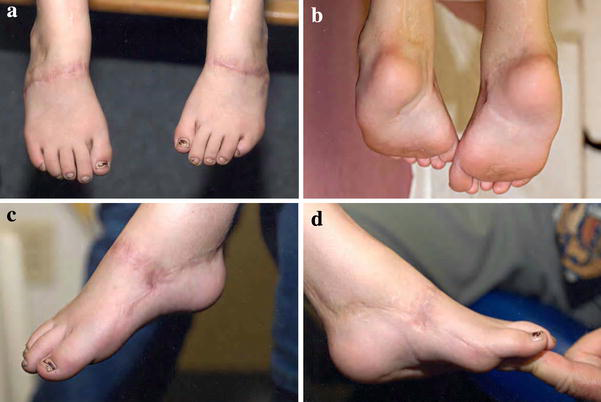
Clinical presentation of a complex rigid foot in a patient with a diagnosis of severely rigid clubfeet, showing scarring from previous surgeries:

Preoperative AP and lateral radiographs demonstrating severe equinus and cavovarus deformity in a patient with a diagnosis of idiopathic clubfoot
A plantigrade foot is optimal for proper lower extremity mechanics in a child with ambulatory potential. Although these types of feet are uncommon, such rigid foot deformities render these feet susceptible to painful calluses, ulcers, difficulty with conventional shoe wear, and potential infection. Several papers have discussed corrections of associated deformities treated with uniplanar supramalleolar osteotomies [1–29]. Deformities, including valgus, varus, equinovarus, calcaneus, tibial torsion, and pure equinus, have all been described, on occasion, as being correctable with supramalleolar osteotomy. Current publications have been confined to the correction of uniplanar deformities, most commonly derotation osteotomy.
The purpose of this article is to describe a surgical multiplanar approach for the correction of these less common but complex rigid foot deformities in children utilizing a multiplanar supramalleolar osteotomy of the tibia as a salvage procedure. This above-the-ankle approach has allowed for avoidance of the commonly encountered scarring and severe structural deformity within the foot itself.
Materials and methods
A retrospective review of 29 multiplanar supramalleolar osteotomies was conducted between October 1983 and October 2005. Two cases were excluded because follow-up was less than 2 years, leaving 27 surgeries in 18 patients in the study. A good result was considered a plantigrade foot on physical exam with follow-up of at least 2 years and no subsequent tibial surgeries. The surgery was deemed a failure if there was a recurrence of the deformity, if there was a nonplantigrade foot at follow-up, or if a repeat supramalleolar osteotomy was performed. All failures were included regardless of the length of follow-up.
The average age at the time of surgery was 5.6 years (11 months–14 years). All feet had a substantial degree of scarring from previous surgeries or burns in addition to the rigid structural foot deformity (Figs. 1, 2). The types of multiplanar deformities noted included 12 equinovarus, four rotational and varus, four rotational and equinus, three rotational and valgus, three rotational and equinovarus, and one equinovalgus (Table 1). The underlying diagnosis of the patients with these complex rigid feet included seven severe rigid clubfeet, five arthrogryposis, two myelodysplasia, one Ellis-van Creveld, one Streeter's, one cerebral palsy, and one severe burn (Table 1).
Data on the 18 patients with the 27 multiplanar supramalleolar osteotomies included in the study
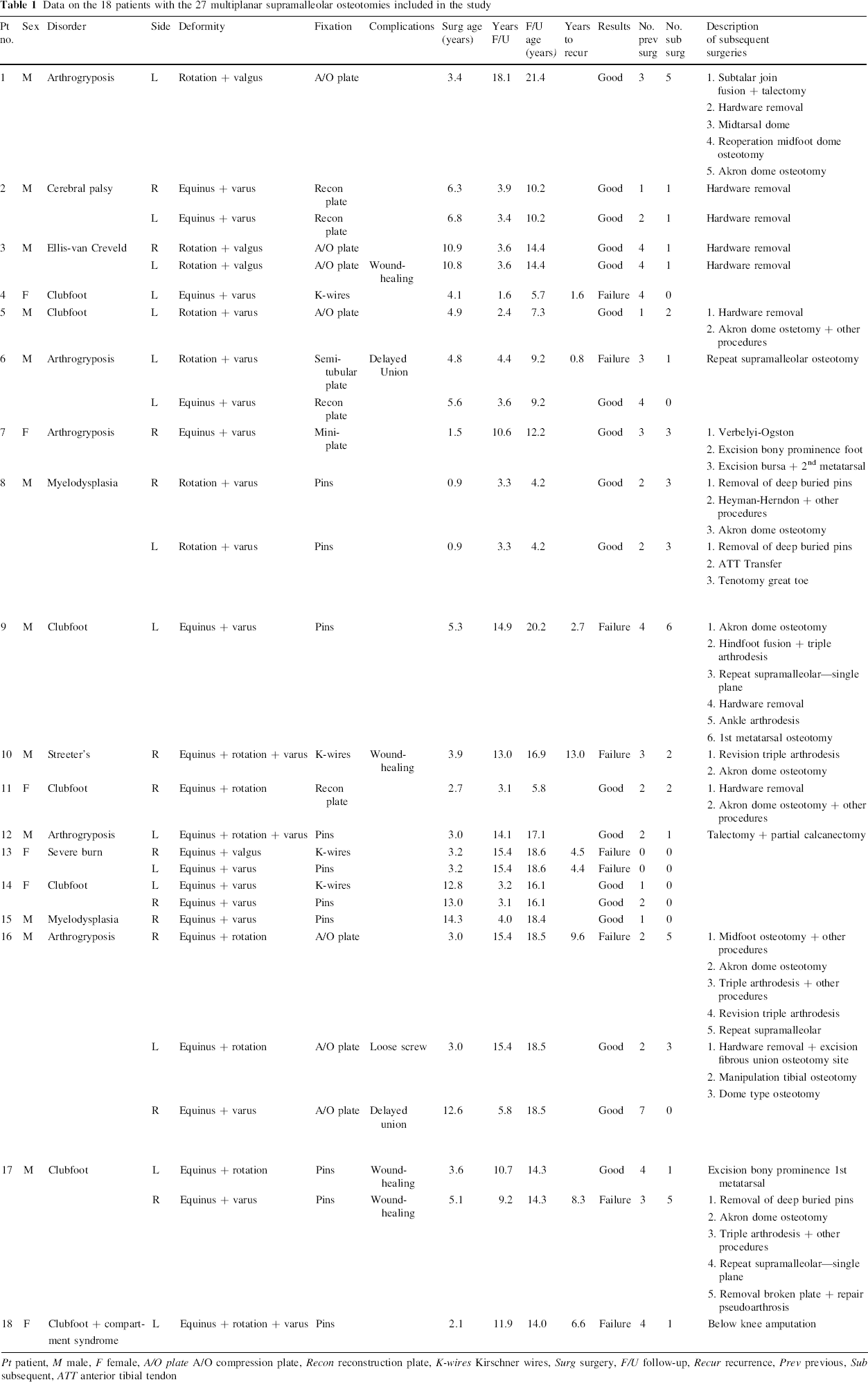
Pt patient, M male, F female, A/O plate A/O compression plate, Recon reconstruction plate, K-wires Kirschner wires, Surg surgery, F/U follow-up, Recur recurrence, Prev previous, Sub subsequent, ATT anterior tibial tendon
Surgical technique
An anterior approach to the distal third of the tibia was performed after a distal fibular ostectomy was performed 5 cm above the distal fibular flare. The distal tibia was exposed over a sufficient distance to allow for insertion of a plate and screws without violating the distal tibial physis. Appropriate anatomically designed wedging and rotation (multiplanar) were fashioned into the osteotomy to compensate for the distal deformity in the foot (Fig. 3). Coronal plane adjustments were used to correct varus and valgus, axial plane adjustments were used to correct internal and external rotation, and sagittal plane adjustments were used to correct equinus and calcaneus. We strongly believe that during the time of correction any rotational deformity should be managed first and then the angular correction subsequently. This allows for more congruous surfaces for apposition prior to fixation. Direct vision of the ultimate foot position (plantigrade) dictated the degree of architectural design at the osteotomy site. Fixation was secured using pins on occasion or, most commonly, a properly conformed plate and screws (Fig. 4). Postoperative care consisted of a well-padded, non-weight-bearing long-leg cast until radiographic union was achieved, usually by 8–10 weeks.
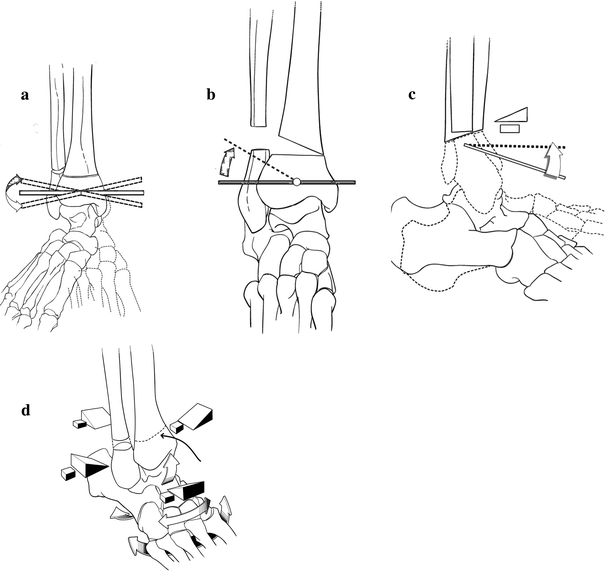
Drawings of multidirectional corrections that are possible:

Postoperative correction on AP and lateral radiographs and lateral weight-bearing radiographs of severe equinus and cavovarus deformity
Results
A plantigrade position of the foot was obtained at the time of surgery in all cases. At the time of follow-up, 18 of the 27 feet maintained their plantigrade correction. These 18 feet were graded as having a successful outcome and were followed an average of 6.4 years (2.4–18.1 years). Fifty-six percent of the feet with a successful outcome (10 feet/18 feet) were followed until the children were at least 14 years of age. The average age at the time of surgery in the successful group was 6.5 years. Nine of the 27 feet were considered failures due to the recurrence of deformity and a nonplantigrade foot. The time to recurrence averaged 5.7 years (9 months–13 years). Four of these patients had a repeat supramalleolar osteotomy, two had other surgeries, and three had no further surgical procedures (Table 1). The average age at the time of surgery in the failure group was 3.9 years. Seventy-eight percent of the feet considered failures (seven feet/nine feet) were followed until they were at least 14 years of age.
Complications from the surgery were few and minor. These included four minor wound-healing problems that all healed, two delayed unions that eventually healed, and one loose screw unaccompanied by any sequalae. One delayed union healed in 3 months and the other in 9 months. No cases of nonunion, growth plate closure, deep infection, or fracture around the hardware or after hardware removal were encountered.
Discussion
Many authors have described using uniplanar supramalleolar osteotomies for deformities in the hindfoot and ankle [1–3, 7–9, 11–13, 17–26, 28, 29]. Wiltse described closing medial wedge supramalleolar osteotomy to realign the ankle in valgus deformity [28]. Others, such as Lloyd-Roberts, Lichtblau, McNicol, and Goldner, used supramalleolar osteotomy to correct equinus and derotate the tibia in equinovarus deformities [4, 5, 7, 9, 11, 14, 16, 20, 24, 29–32]. Abraham utilized the approach to correct ankle valgus in patients with myelomeningocele [2]. Pearce presented a small series of hemophilic arthropathy patients treated for valgus deformity by supramalleolar osteotomy [18]. Many authors have utilized supramalleolar osteotomies to derotate the tibia alone in torsional deformities [4, 5, 7, 9, 11, 14, 16, 20, 24]. Percutaneous supramalleolar osteotomies have been performed for rotational deformities in cerebral palsy [9]. Supramalleolar osteotomy is being described here as a salvage procedure for the treatment of the uncommon complex rigid multiplanar hindfoot deformities with previous postoperative scarring or scarring from severe burns.
Many authors have looked at the use of Ilizarov external fixators for the correction of complex foot deformities. Although this is a valid option for correction, we have shown the use of a supramalleolar osteotomy can achieve excellent results with significantly fewer complications and an arguably easier procedure. Kocaoğlu et al. [33] had a 100% complication rate using the Ilizarov technique. Paley also had 20 minor and major complications in 18 feet requiring 19 secondary procedures in 13 patients [17].
It has been previously suggested that multiplanar corrections with supramalleolar osteotomies using internal fixation was not feasible [23]. It is clear from this study that multiplanar correction through appropriate architecturally designed osteotomy can compensate for the severe distal foot deformity and result in a plantigrade position. Minimal complications have been encountered. The most significant sequelae encountered were recurrences with growth and time, and it is appreciated that additional recurrences in this group will likely appear. In this series, these recurrences were classified as failures, but repeat salvage multiplanar supramalleolar osteotomies can be employed with reasonable results to be expected.
Potential cases requiring multiplanar correction are relatively uncommon in the general population and are reflected in this relatively small number of cases (27 feet). However, this group is clearly among the most difficult in management due to the severe, complex rigid deformities, most with extensive scarring from previous operative attempts at correction with accompanying severe structural deformity. By moving above the ankle to a site in the distal tibia, multiplanar correction into a plantigrade position was achieved in all feet at the time of surgery. The younger age at which many of the surgeries were performed likely resulted in the number of recurrences, 9 of 27 (33%) due to the remaining growth. Repeat supramalleolar osteotomy can usually be safely performed for recurrences.
The authors recognize the limitations in this study. Some cases did have shorter follow-up, and it is impossible to predict future outcomes based on this data. However, the goal of the surgery is to achieve a plantigrade foot at the time of surgery, which was done in each case, and maintain the plantigrade foot at 2 years’ follow-up. We also recognize the limitation of having numerous diagnostic categories in our paper. However, it was not the goal of the paper, nor was it possible, to extrapolate reasonable prognostic data based on each diagnostic etiology due to the limited number of cases in each group. We simply wanted to show one solution for obtaining a plantigrade foot for patients with a previously operated on, complex, rigid, scarred foot. The benefit of this procedure is that subsequent supramalleolar osteotomies can be done to correct the recurrences.
Conclusion
Based on this study, multiplanar supramalleolar osteotomy appears to be a reasonable, safe, and effective salvage surgical option for severely scarred and complex rigid foot deformities.
Footnotes
Acknowledgments
The authors would like to express their appreciation to Tom Campbell, Medical Illustrator, and Martin S. Dicintio, Assistant Research Coordinator, Pediatric Orthopedic Research, Akron Children's Hospital, for their assistance in this project.