
Abstract
Abstract
Introduction
We investigated the clinical and radiological outcome of proximal femoral osteotomies in children using the Richards hip screw. We also describe previously unreported techniques used in the insertion of the screw to aid satisfactory correction of the neck shaft angle and medialisation.
Methods
Seventy-two children undergoing 81 proximal femoral osteotomies under the care of the senior author over a 10-year period were reviewed.
Results
For the primary procedure, there was an overall complication rate of 5%. This included two (2.5%) cases requiring re-operation. There were no fractures and no long-term complications. For subsequent removal of the metalwork, the complication rate was 5%, with a re-operation rate of 1%.
Conclusion
We conclude that the Richards hip screw is a safe, atraumatic and easy-to-use method of fixation for proximal femoral osteotomies in children, with lower complication.
Introduction
Proximal femoral osteotomy (PFO) is a widely performed procedure in paediatric orthopaedics. It is used in the treatment of conditions such as developmental dysplasia of the hip (DDH) [1], Legg-Calvé-Perthes disease (LCPD) [2–6], slipped upper femoral epiphysis [3, 7–11] and cerebral palsy (CP) [12–14].
A wide variety of implants have been used for fixation. These include the Coventry screw [3], blade plate [15–17], crossed Steinmann pins [1], external fixation [18] and, more recently, a two-piece sliding hip screw construct, such as the Richards hip screw [17].
The blade plate is sometimes considered to be the standard implant for fixation [15, 19, 20]. However, studies have shown that this technique has serious complications, including infection (2.5%), loss of fixation (1%), wound breakdown (1%) and, most notably, fracture (1–4.5%) [15, 17]. The removal of blade plates has also been demonstrated to have a significant morbidity, including fracture (1%) and wound infection (3%) [21]. Sliding hip screws (e.g. the Richards paediatric and intermediate hip screw) are a more recent option for the fixation of PFO. Their increasing popularity relates to the familiarity and the safety profile of a similar adult device for hip fractures [17]. The potential benefits of this implant compared with the blade plate are a gentler technique for insertion and removal, and greater intra-operative flexibility in the adjustment of the neck shaft angle. However, a previous paper has demonstrated similar complication levels to that of blade plates [17]. It has also been suggested that hip screw fixation requires the increased use of hip spicas post-operatively and results in lateralisation of the femoral shaft, an undesirable feature.
The routine removal of metalwork after PFO is common practice, as approximately 40% of patients may require total hip replacement in later life [22]. However, this is often associated with significant complications, with a rate of 5.6% documented for blade plate removal post-PFO [23]. The complication rate of hip screw removal has not been previously reported.
We present the results of proximal femoral osteotomies performed under the care of one consultant surgeon over a 10-year period. The aim was to establish the incidence of complications and outcomes following PFO in children using the Richards hip screw. We also describe novel surgical techniques for the insertion of the hip screw to allow greater correction of the neck shaft angle and medialisation. Secondly, we document the complications of the subsequent removal of the hip screw.
Methods
We retrospectively reviewed the clinical notes and radiographs of all children aged 16 years or less who underwent proximal femoral osteotomies under the care of the senior author over a 10-year period. We excluded the small number of cases who underwent fixation by means other than the Richards hip screw. Patients with less than 2 years follow-up were also excluded. Patient diagnosis and demographic details were recorded. Pre-operative radiographs were analysed, and neck shaft angle and Reimer's migration percentage were recorded [24]. Hard copy fluoroscopy was used for follow-up rather than conventional radiographs because the radiation exposure is greatly reduced [25, 26].
Operative details assessed included the type of osteotomy, i.e. varus, valgus, rotational, shortening or a combination. Blood loss was recorded as a percentage of the estimated total circulating volume (calculated as weight in kg multiplied by 80). The use of spica casting after operation was also documented.
The length of time spent in plaster and the follow-up duration were recorded. Post-operative radiographs were analysed in the same manner as the pre-operative films. All complications, and subsequent outcomes, were recorded.
Operative technique
Patients were placed supine on the operating table. Conventional C-arm fluoroscopy was used. Arthrography was performed in all cases prior to the main procedure.
A standard postero-lateral approach to the femur was used in all cases. Vastus lateralis was elevated anteriorly, the femur being approached along the intermuscular septum.
The guide wire was inserted along the axis of the femoral neck under image intensifier control. A lateral view of the femoral neck was obtained by flexing the hip 90°. This wire, defining as it does the axis of the femoral neck, was used as the proximal reference for estimating the degree of anteversion present.
The posterior condylar tangent on computed tomography (CT) would define the rotational position of the distal segment absolutely; the closest that we can approach this intra-operatively is to assume that the axis of the tibia (with the knee flexed 90°) bears a constant relationship to the posterior condylar tangent. It is this assumption that underpins Staheli et al.'s methods of clinical rotational measurement [27]. This works because the axis of the flexed normal tibia is close to perpendicular to the posterior condylar tangent. The pre- and post-osteotomy degree of anteversion can be estimated by comparing the axis of the guide wire to the perpendicular of the axis of the tibia with the knee flexed 90°. The intention was to return the femur to a physiological degree of anteversion. The bone on either side of the osteotomy is marked with a shallow drill or saw mark for quick reference during the operation.
The osteotomy and fixation technique did vary from standard surgical techniques. Particular attention was given to avoid unnecessary stripping of the periosteum. The periosteum was incised in an H-shape and was elevated only in the immediate vicinity of the osteotomy. Plates were applied on top of the periosteum.
The philosophy is that the closer the osteotomy is to the hip joint, the greater is the effect on hip function. The aim, therefore, was to perform the osteotomy in the intertrochanteric area whenever possible. A secondary advantage at this level is that the psoas and gluteus maximus are not uncoupled, both being on the same side of the osteotomy. Consequently, there is a lesser tendency for the proximal fragment to rotate around the implant.
Abduction/valgus osteotomies were performed using a closing wedge or reversed hemi-wedge technique, according to limb length considerations. The Richards hip screw technique was standard, as illustrated in standard texts and the product literature.
In CP hip dysplasia, one is often faced with the necessity of performing a large varus/derotation correction of the femur, when there is already an adduction contracture. To meet this challenge, a radical adductor and psoas release is undertaken as a preliminary, followed by a varus osteotomy incorporating a degree of shortening (Fig. 1a).
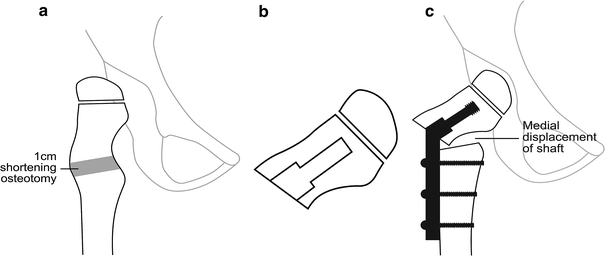
To obtain the angulation required, it is necessary to insert the screw and barrel of the hip screw through the face of the osteotomy surface [28, 29] (Fig. 1b). The osteotomy is performed prior to guide wire insertion. The guide wire is inserted under image intensification. The entry point is on the face of the osteotomy. To obtain a lateral view, it is necessary to rotate the upper fragment 90° with forceps. Because of the soft-tissue attachments bridging the osteotomy site, it is difficult to rotate this fragment until the assistant has lifted the leg into the position it would have occupied if the femur were intact. Once correct positioning of the guide wire is confirmed, reaming is performed, followed by lag screw insertion. An appropriate plate is chosen to give the required neck shaft angle.
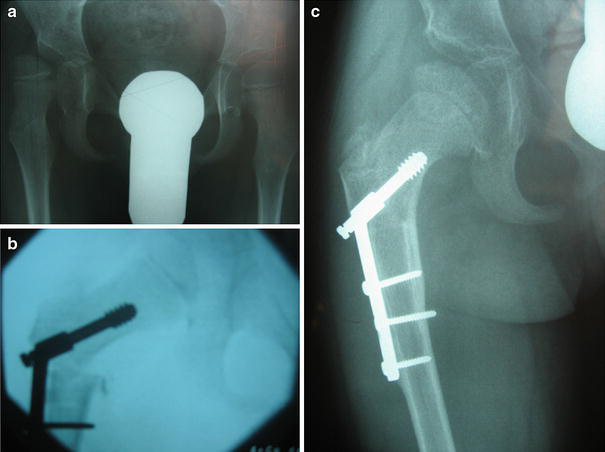
With the osteotomy reduced, there is beneficial medial displacement of the femoral shaft, which relaxes the adductors further. The plate is fixed to the shaft with screws (Fig. 1c). An example of this technique is shown in Fig. 2a–c.
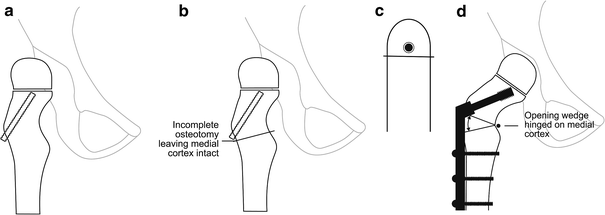
For varus containment osteotomies in LCPD, a different technique was used to give an open-wedge osteotomy. Arthrography was carried out with Urografin 150 to confirm containment, the angle of abduction necessary to produce containment (the anticipated osteotomy angle) and the presence of at least 20° of ‘abduction reserve’ beyond the containment position.
Under image intensifier control, a guide wire was inserted centrally in the femoral neck in anterior-posterior and lateral views. After reaming, a lag screw was inserted a few mm proud of the lateral cortex (Fig. 3a). A single-cut incomplete osteotomy is carried out immediately below the insertion point of the lag screw, producing a configuration resembling the Greek letter omega, ω. The intention is to leave the medial periosteum intact and bend the medial cortex like the spine of a book (Fig. 3b, c). This confers stability to the osteotomy, particularly in the axis of the hip screw. The osteotomy is continued medially only to the point where adduction of the leg over the other results in the opening of the osteotomy. A plate with the appropriate barrel angle is inserted on top of the periosteum of the distal fragment (Fig. 3d). The containment and abduction reserve are checked and, if necessary, the plate can be changed for another barrel angle.
In DDH, bony deformity becomes increasingly significant with increasing age. Modest varus and de-rotation are indicated, together with shortening to reduce the risk of avascular necrosis. The compression hip screw technique was standard, as illustrated in the product literature.
It is the practice in our unit to routinely remove metalwork following PFO at 1 year from the time of original surgery; therefore, all of the above patients remaining under our care underwent this procedure. This was carried out through the original incision. All patients were encouraged to weight-bear following hardware removal and none were immobilised.
Results
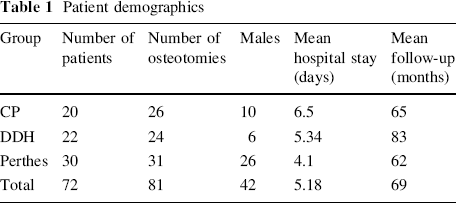
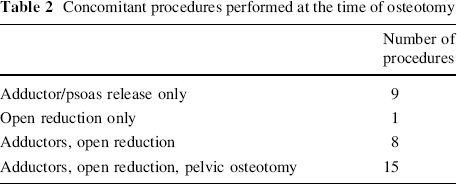
During the study period, 93 patients were identified, undergoing a total of 102 proximal femoral osteotomies. Of these, 72 patients, undergoing 81 osteotomies, had traceable notes and radiographs (Table 1). The patients fell into three groups: neuromuscular/CP, DDH/syndromic and LCPD. The mean follow-up time was 69 months, the minimum being 32 months. The type of osteotomy performed varied according to the diagnostic groups. LCPD children had either a varus containment osteotomy or a valgus osteotomy for painful hinge abduction. Those with DDH and CP had a combination of varus, derotation and shortening osteotomies. Concomitant procedures performed in the same theatre session are shown in Table 2. The radiographic outcome is shown in Table 3. The mean change in the neck shaft angle was 34°. The mean decrease in migration percentage was 43%.
Patient demographics
Concomitant procedures performed at the time of osteotomy
Radiographic outcome

The mean values are shown for each group
MP migration percentage, NSA neck shaft angle
The mean intra-operative estimated blood loss was 9% of the total circulating volume. If those patients who had other major procedures (i.e. pelvic osteotomy) carried out concomitantly were excluded, then the mean blood loss was 7%. Transfusion requirements in the peri-operative period were also recorded.
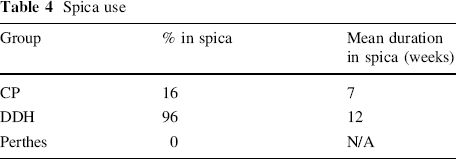
Spica use and duration is shown in Table 4. The majority of patients who had a spica applied were in the DDH group, and had undergone concurrent open reduction. No patients with LCPD required the use of a spica. The average duration of spica use was 7 weeks for the CP group and 12 weeks for the DDH group.
Spica use
Complications
There were no deaths during the study period. The morbidity is shown in Table 5. The most serious complication occurred 2 weeks after a derotation osteotomy. The patient was readmitted with increased discomfort; radiographs showed that the upper fragment had rotated around the screw and was loose. It was, therefore, not feasible to retain the existing fixation and it was removed. The osteotomy was then repositioned and it was fixed with a standard AO tibial plate, contoured to fit the upper femur. The patient remained non-weight-bearing until bone union and had no further problems.
Complications of hip screw insertion

All of our patients received our standard antibiotic prophylaxis of cefuroxime on induction, with two subsequent doses of cefuroxime on the ward in the post-operative period. No patients developed deep wound infections, although two patients (2.5%) did require oral antibiotics for superficial wound infections.
There were no fractures. No patients developed nerve palsies. No patients developed wound breakdown. All osteotomies united without cause for concern. All complications were resolved at the end of the treatment episode.
Due to a small number of patients moving elsewhere, 75 hip screws were removed. The average time of removal was 14 months from the time of original surgery. Of the 75 operations, there were five complications, one of which required re-operation (Table 6). This gives an overall complication rate of 6% and a re-operation rate of 1%. There were no fractures. Two patients developed a superficial infection, requiring oral flucloxacillin. On attempting to remove the metalwork in one patient, the screw had cold-welded to the barrel of the plate. The device was removed by rotating the plate as if it were a spanner. No complications ensued. The metalwork was unable to be removed in one patient due to the stripping of the heads of the screws, and the decision was made to leave the hip screw in situ. One patient developed a wound haematoma, which was evacuated surgically. This had no long-term sequelae. The majority of patients were discharged the day after surgery. No patients required post-operative transfusion.
Complications of hip screw removal

Discussion
This is the largest reported series of proximal femoral osteotomies in children using the Richards paediatric and intermediate hip screws. Two previous studies [15, 17] have reported results of PFOs using hip screws and/or blade plates. These report remarkably similar overall complication rates of 9% [17] and 8.9% [15]. Our rate of 5% compares favourably. Hau et al. reported 13 complications in a mixed series of 164 PFOs fixed with either a blade plate (108/164) or a hip screw (56/164). Ten of the 13 complications required re-operation. Beauchesne et al. reported 157 PFOs fixed with blade plates, with 14 complications (seven fractures, seven re-operations, four casts required). Hau et al. reported a 0% fracture rate with the 56 hip screw osteotomies, and our study backs up these findings. This would suggest that the hip screw is less traumatic than a blade plate to insert into what can be very gracile, osteopenic bone, particularly in CP.
The use of a hip spica post-operatively is a contentious issue. The decision to use a spica is not just based on the perceived stability of the fixation. Many of the patients in this study underwent pelvic osteotomy and/or soft-tissue release at the same time as a femoral osteotomy. These, therefore, required spica casting to maintain the optimal position of the hip. The vast majority of patients that underwent PFO as a sole procedure were simply mobilised non-weight-bearing. None of these had subsequent problems with fractures or loss of position of the proximal fragment. It has been stated that the use of a fixed-angle blade plate can avoid the need for a hip spica [17]. We believe that the same can be said of the hip screw.
The only complication in the study requiring revision was due to the rotation of the position of the proximal fragment in a subtrochanteric osteotomy. Osteotomies (or fractures) in the subtrochanteric area are prone to flexion of the upper segment due to the uncoupling of the psoas (flexor attached on the upper fragment) and gluteus maximus (extensor attached to the lower fragment). Osteotomies and fractures in the intertrochanteric area are not prone to this problem, as flexors and extensors are not decoupled. The majority of osteotomies in this series were intertrochanteric. This drawback of the hip screw can be avoided by the use of a second screw placed into the proximal segment through the proximal hole on the plate [30] or separately. We, therefore, recommend this for subtrochanteric osteotomies.
It has been thought that a drawback of the hip screw is that medialisation of the femoral shaft cannot be performed. Lateralisation of the shaft is often undesirable, as it widens the perineum and malaligns the mechanical axis. However, lateralisation is avoided, and medialisation is achieved, if the surgical technique is modified, as we have previously described in this paper [28, 29]. In large varus corrections, usually in CP, the best policy is to divide the bone in the intertrochanteric area. Then, the guide wire is inserted into the face of the osteotomy and up the femoral neck, prior to standard reaming. Then the hip screw, followed by the barrel of the plate, is inserted through the osteotomy surface of the proximal fragment. This has the effect of medialising the shaft. This is demonstrated in Fig. 1. In our study, there was no case of wound breakdown. We believe that this is attributable to the low profile of the hip screw compared to the blade plate. Many of our patients in the CP group are prone to wound problems, as they can be small for their age and malnourished.
The question of whether to remove metalwork after bony union in a paediatric population is a contentious one, with arguments both for and against [31–33]. Post-operative complications have ranged from 5 to 11%, although these were in a mixed-case group of patients, not just PFOs. Becker et al. [21] reported an overall complication rate of 5.6% in a study of blade plate removal post-PFO. This included a major complication rate of 2% and a fracture rate of 1%.
The policy in our unit is to routinely remove metalwork after 1 year following PFO. This is for two reasons. Firstly, the metalwork can, in some instances, be felt through the skin and cause discomfort. However, this does occur to a lesser extent than the blade plate, with its bulky lateral profile. Secondly, many of these patients will require hip surgery when they are adults, which would be significantly complicated by the presence of metalwork in the proximal femur. Removal of the metalwork a year after surgery is far easier than removing it in adult life, when it is buried in bone. The findings of this study demonstrate that they are safe to remove, with a low overall complication rate, and in particular, a 0% fracture rate.
Conclusions
We find that the Richards paediatric and intermediate hip screws are easy to use, versatile implants for use in proximal femoral osteotomies in children. They are relatively atraumatic to insert, allowing intra-operative flexibility in the selection of the final fixation position. When used to fix an osteotomy without concurrent procedures, a hip spica can usually be avoided. By appropriate modification of the surgical technique, medialisation of the shaft can be achieved if required. A limitation of the device is the risk of rotation of the proximal fragment around the screw in subtrochanteric osteotomies, which can be avoided by the addition of an anti-rotation screw. We also conclude that the routine removal of hip screws can be safely advocated following proximal femoral osteotomy (PFO).