
Abstract
Background
Studies have shown that when using a spica cast following hip surgery in children, there are associated complications such as soiling, pressure sores, and osteopenic fractures.
Methods
Charts were retrospectively reviewed for all patients who had undergone hip surgeries by one surgeon at one institution between 1999 and 2005. The method of post-operative immobilization (spica cast or abduction pillow) and complications were recorded for each patient.
Results
There was a total of 32 patients. Of these, 11—all of whom had a diagnosis of developmental dysplasia of the hip—were treated using a spica cast. In the 21 patients treated in an abduction pillow, 4 (19%) were switched to a spica cast for the following reasons: (1) distal femoral fracture as a result of vigorous resuscitation during a choking episode, (2) parental preference, (3) for added immobilization over concern of implant loss of fixation, and (4) concern of migration of the hip, which again migrated after being changed to a spica cast and eventually required a pelvic osteotomy.
Conclusion
It is our opinion that only one of these complications in the children treated with an abduction pillow (the case of possible implant migration) may have been avoided if the child had originally been placed in a spica cast. The child who was successfully resuscitated after a choking incident weeks after the surgery may have had a worse outcome if it had been in a spica cast. This incident occurred at home and the abduction pillow was easily and quickly removed to allow resuscitation. An abduction pillow is a welcome alternative to a spica cast following hip surgery for many patients with neuromuscular and syndromic conditions. However, in children with osteopenic bone at risk for implant failure and in children with unstable hip reductions, a spica cast may be preferable.
Introduction
Children with neuromuscular disorders and other genetic syndromes undergo hip surgery for many reasons, such as hip subluxation, dislocation, and acetabular dysplasia. Femoral and/or pelvic osteotomies, often in conjunction with open hip reduction, followed by spica cast immobilization are the main method for accomplishing this surgically in the immature patient [1–4].
Osteopenic disuse fractures possibly related to the spica cast following surgery have been reported in up to 6 of 21 (29%) non-ambulatory cerebral palsy (CP) patients [5]—Mubarak et al. [1] reported their occurrence in 1 of 11 CP patients (9%), Pritchett [6] in 9 of 50 CP patients (18%), and Stasikelis et al. [7] in 16 of 79 CP patients (20%). Miller et al. [8] described there being no fractures in 51 patients with dysplastic spastic hips after surgery, followed 2–3 days later by physical therapy with no form of immobilization. Decubiti ulcers have been reported in 7 of 76 (9%) patients by Stasikelis et al. [7] and 0 of 14 (0%) by Sankar et al. [9]
In order to decrease the risks associated with spica casts, all patients with no diagnosis of developmental dysplasia of the hip (DDH) were placed in an abduction brace post-operatively. We present our experience using abduction pillows post-operatively following hip surgery.
Materials and methods
All patients with who had undergone hip surgery requiring post-operative stabilization between 1999 and 2005 by one surgeon at our institution were identified retrospectively. A total of 33 patients were identified who were treated with either an abduction pillow and knee immobilizer or a spica cast. Of these 33, 1 had no adverse outcomes, but we were unable to obtain at least 5 months of follow-up records. Since other studies demonstrate that most peri-operative events occurred within 3–5 months of the surgery [7], only charts with at least 5 months follow-up were included in the study. Of the remaining 32 patients, 21 underwent hip surgery and were treated with an abduction pillow and 11 were treated post-operatively with a spica cast. All records were searched for adverse outcomes, including decubiti ulcers, fractures, death, or dislocations.
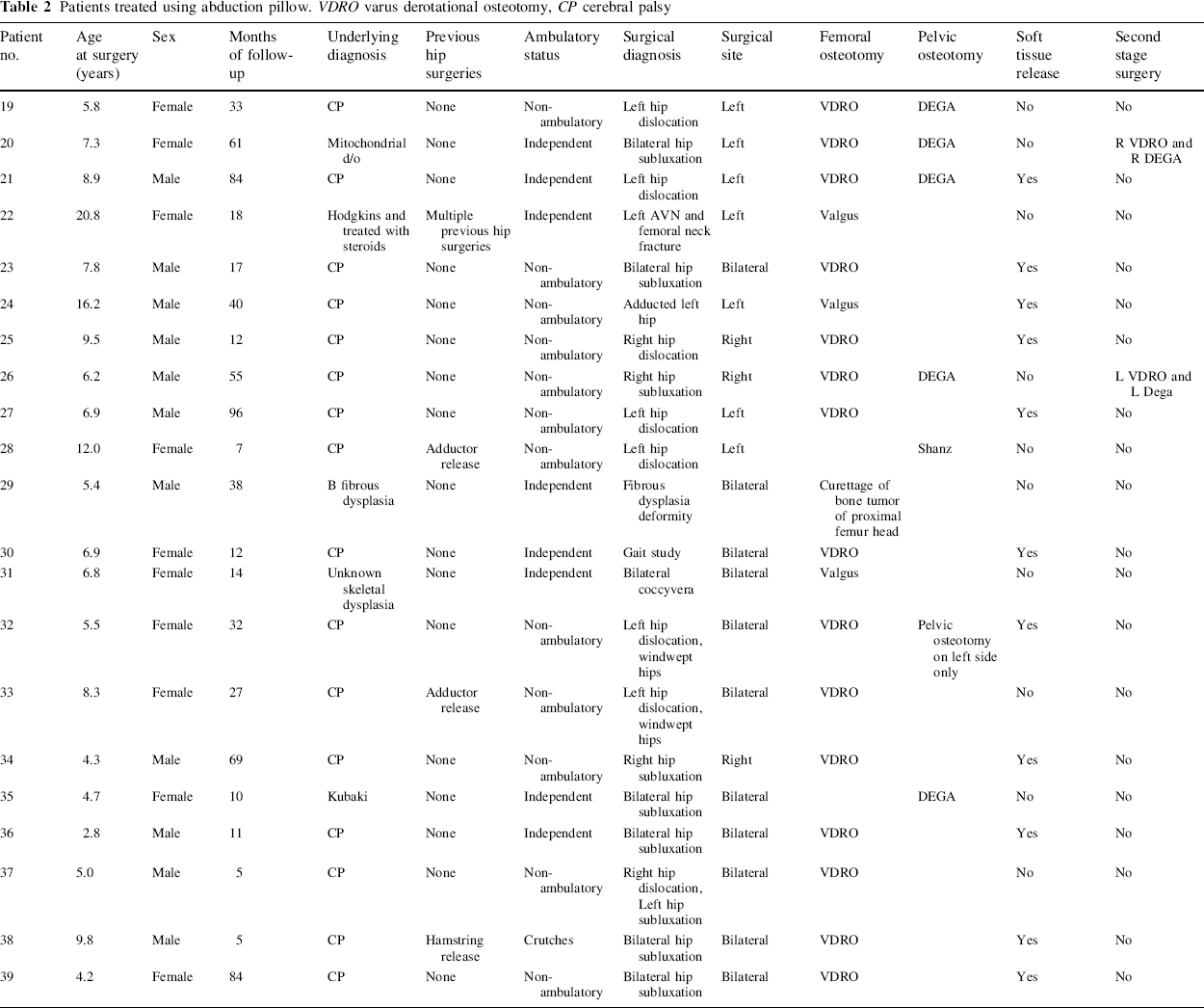
Of the 21 patients who were treated using an abduction pillow and a knee immobilizer on the operated leg, there were 32 hips that had a femoral and/or pelvic osteotomy (Table 1). The average age at treatment was 7.9 years (5.8–20.8 years) and average follow-up was 34.7 months (3–96 months). Of these 21, 16 patients had CP and 5 had genetic syndromes. A total of 2 patients underwent two-stage reconstructions with one hip being operated on 2–3 weeks before the other hip, with an abduction pillow used in the interim.
Patients treated with spica cast. VDRO varus derotational osteotomy, CP cerebral palsy
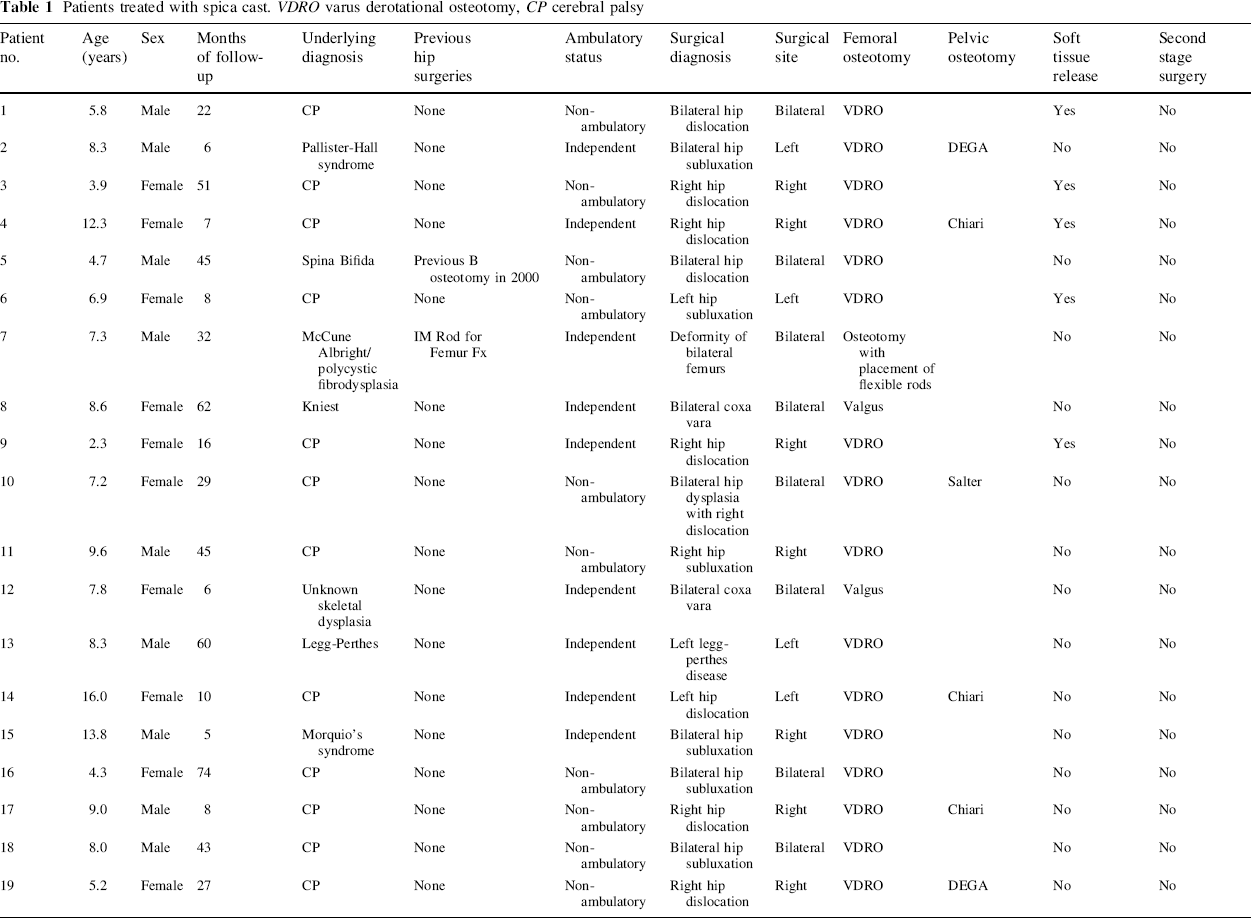
Of the 11 patients treated using a spica cast, every one had a diagnosis of DDH and was operated on with a pelvic and/or femoral osteotomy. The average age of the patients was 2.3 years old (0.3–4.8 years) at the time of surgery. The average follow-up time was 32.5 months (8–84 months) (Tables 2, 3).
Patients treated using abduction pillow. VDRO varus derotational osteotomy, CP cerebral palsy
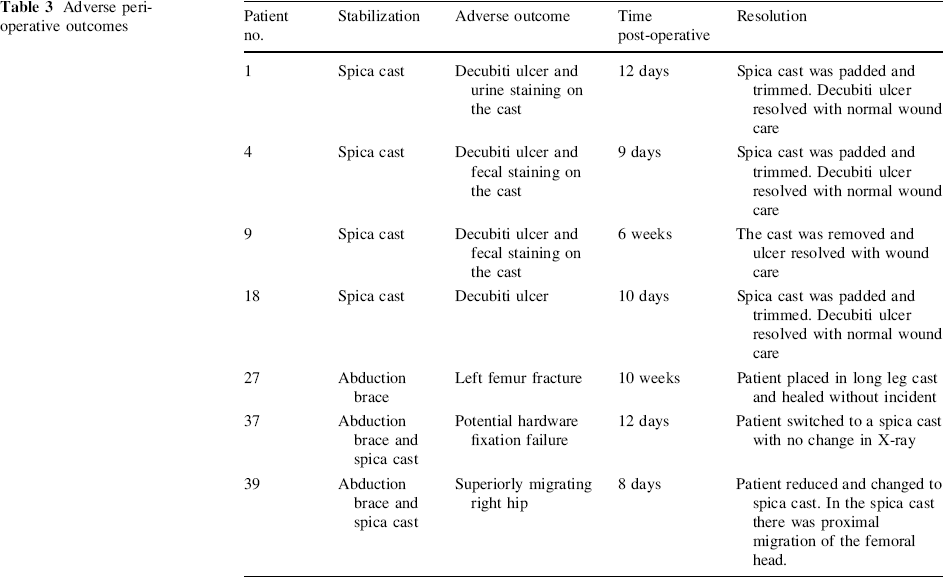
Adverse peri-operative outcomes
Results
Of the 21 patients who were treated using an abduction pillow (Fig. 1) after surgery, 17 experienced no complications during the peri-operative period. Patient 20 was a 9.8-year-old male with CP who switched from the abduction pillow to a spica cast 8 days after a varus derotational osteotomy (VDRO), because the mother stated that the knee immobilizers were sliding down the patient's legs and were difficult to maintain. The hips were well located on X-ray before and after changing to a spica cast.

Abduction Pillow
One patient with quadriplegic CP sustained a distal femoral fracture 10 weeks after the surgery. This patient was 6.9 years old at the time of the surgery and non-ambulatory; 10 weeks after surgery, while being stabilized with an abduction pillow, the patient was noted by his mother to be choking on a hotdog. During forceful manipulation to dislodge the hotdog, the patient sustained a left distal femoral fracture. The patient was converted to a spica cast and the hip surgery and femur fracture healed without incident.
Another patient, a 5-year-old male with CP was immobilized using an abduction pillow following VDRO. A potential loss of implant fixation was noted on X-ray at his 2-week follow-up appointment. The patient was changed to a spica cast, and on repeat X-ray there was no radiographic change in implant position. The spica cast was removed 6 weeks post-operatively and the implant remained in place with the VDRO well healed.
One week after performing bilateral VDRO on a 4-year-old non-ambulatory patient with CP, it was noted on radiographs that the right hip was superiorly migrating. The next day, the patient underwent general anesthesia, the hip was reduced in a closed manner, and a spica cast was placed. And 2 days later, X-rays showed that the femoral head was again migrating superiorly. A Dega pelvic osteotomy was performed after a further 3 days, and the patient was placed in a spica cast after the surgery. The hip then remained reduced.
In the 11 patients treated with a spica cast, 10 experienced no adverse events. Patient number 25 had a wound infection 2 weeks post-operatively with an elevated CRP of 3.0. The patient was administered IV antibiotics and the infection resolved. Her femoral head was noted to be migrating laterally on X-ray 3 months post-operatively, and a repeat pelvic osteotomy with spica stabilization was thus performed. The hip then remained reduced with no further complications.
Discussion
Many children with CP and other genetic conditions require hip surgery for subluxated and/or dislocated hips. Due to their many co-morbidities, complications following such surgery are common. There have been many recognized complications associated specifically with spica casts, such as osteopenic disuse fractures and, rarely, vessel [10] or nerve [11] damage along with perineal care issues that the cast presents. Decubiti ulcers related to the spica cast have been reported in 0–9% of patients with CP following hip surgery and spica cast application [7, 9].
Osteopenic disuse fractures, mostly distal femur/proximal tibia, are associated with application of a spica cast following surgery. Sturm et al. [5] observed fractures in 6 of 21 non-ambulatory CP patients who had been operated on for subluxed or dislocated hips and treated with a spica cast. Shea et al. [12] reported no fractures in 15 patients with CP who underwent a Pemberton pericapsular osteotomy to treat a dysplastic hip. In a study by Mubarak et al. [1], 1 of 11 patients sustained a fracture after pericapsular acetabuloplasty and spica stabilization, and Root et al. [13] observed femoral fractures in 3 of 31 patients with CP who had an open reduction, pelvic osteotomy, and femoral osteotomy with shortening with stabilization using a spica cast. Of 47 patients with spastic CP, Brunner et al. [3] observed 2 to sustain a femoral fracture within 3 months of surgical reconstruction of a dislocated or subluxated hip stabilized using a spica cast.
Miller et al. [2] has advocated a routine of physical therapy starting 2 days after pre-ilial pelvic and femoral osteotomy surgery. Of his 51 patients treated in this manner, 1 was placed in a spica cast due to instability of the hip and had a fracture immediately after the cast was discontinued, and 1 had a fracture while getting out of bed 4 weeks after surgery. At a mean follow-up of 34 months, two hips in 2 patients had redislocated, requiring repeated surgery. Two hips remained subluxated and asymptomatic.
To the best of our knowledge, there has been no study examining the use of an abduction pillow after surgery about the hip. This study presents our experience with selective use of an abduction brace in all patients requiring hip stabilization post-operatively; excluding patients with DDH, who were treated in spica casts in order to have greater stabilization.
In our experience, we had 2 patients who had an adverse complication that occurred only while in the abduction pillow. One patient sustained a distal femoral fracture 10 weeks after surgery while his mother was vigorously beating on his back trying to stop him from choking. There is a good likelihood that this fracture would have occurred with or without the recent surgery and abduction pillow. Another child had partial loss of fixation of the hardware in the abduction pillow. This is the one child who very well may have done better if he had been placed in a spica cast immediately; however, the VDRO went on to heal uneventfully in acceptable position.
An additional patient had superiorly migrating hip in the abduction pillow, which was then treated with closed reduction and spica cast application. The hip again migrated superiorly in the spica cast and went on to have a pelvic osteotomy. This complication was most likely a failure of the surgery itself, in that a pelvic osteotomy at the time of the index surgery may have prevented hip migration post-operatively, regardless of post-operative immobilization.
This paper has limitations. Inherent to a retrospective study, the patients were not randomized. The numbers of patients are modest, and it is possible that larger numbers would show different results. The study does not look at the use of an abduction brace for developmental dysplastic hips in otherwise normal children, so these findings are not necessarily applicable to that population. Our findings suggest that the use of an abduction pillow and knee immobilizer or a spica cast following hip surgery in children with neuromuscular and syndromic conditions is generally effective and safe. Selected patients, such as those with poor bone quality in whom implant failure is a risk or those cases of an unstable hip reduction, may do better if treated using a spica cast. Overall, parents and medical staff were much happier caring for children in an abduction pillow and knee immobilizer for many reasons, including perineal care and ease of movement because of the weight of the cast.