
Abstract
Purpose
Late-onset Perthes’ disease is diagnosed after 9 years of age. Conservative treatment and conventional surgical techniques have limited ability to reduce the pressure in the joint or change the shape of the femoral head. We used a combination of soft tissue release and joint distraction with a hinged mono-lateral external fixator for these patients. Ten of our patients reached skeletal maturity and were evaluated.
Methods
Clinical assessment included: Harris hip score, hip range-of-motion (ROM), limb length discrepancy, and the Oxford hip questionnaire for pain and function. Radiographic assessment included: Sharp transverse acetabular inclination, the uncoverage percentage, the epiphyseal index before surgery (modified Eyre–Brook), at frame removal, and, at last follow-up, the epiphyseal quotient (of Sjovall) and the Stulberg classification.
Results
Our study included eight boys and two girls (mean age at surgery 12.3 years, range 9.4–15.1, mean age at last follow-up 18.1 years, range 15.2–22.8). The mean follow-up was 5.7 years (range 4.3–7.8). The mean Harris hip score was 86.3/100 (range 48.5–96); one patient had <85 points. The hip ROM was slightly limited in most patients, and seven patients had limb shortening between 1–4 cm. The mean Oxford hip questionnaire score was 17.4/60 (range 12–31). The mean Sharp transverse acetabular inclination of the affected side was 42° (range 36–54) compared to 39° for the unaffected side (P = 0.045). The mean uncoverage percentage was 37% (range 27–47) compared to 20% for the unaffected side (P = 0.017). The mean epiphyseal index was 0.71 (range 0.31–0.92) before surgery, 0.79 (range 0.50–0.93) at frame removal (P = 0.012), and 0.72 (range 0.51–0.89) at last follow-up (P = 0.646). The epiphyseal quotient for the eight unilateral cases was 0.72 (range 0.49–0.91), and the Stulberg classification was type III for three cases and type IV for seven.
Conclusion
Patient satisfaction for function and pain following the combined procedure was good. Radiographic parameters did not change significantly. This should be regarded as a salvage procedure.
Introduction
Perthes’ disease is defined as being of late onset when it is first diagnosed in patients older than 9 years of age. Older age at initial presentation carries a less favorable prognosis—rapid deterioration of the joint and early arthritic changes are common [1]. These patients may develop a saddle-shaped subluxating femoral head that cannot be contained in the acetabulum. Since conservative treatment does not change the shape of the femoral head or affect joint congruency [2–10], different surgical treatment options have been proposed, including varus osteotomy (which may increase the incongruency) and valgus osteotomy (which may succeed in unloading the deformed part but may increase the subluxation without influencing the basic avascular process) [11–13].
Acetabular lateral shelf, Salter, Chiari, and triple osteotomies are considered salvage procedures at this age group that aim to reorient or increase the size of the acetabulum and produce more support to the femoral head [14–18]. A newer approach to the disease involves intraepiphyseal femoral head osteotomies, but no long-term results are available to date [19].
For the last several years, we have been using a combination of soft tissue release and joint distraction with a hinged mono-lateral external fixator to salvage the hip in severe late-onset Perthes’ disease. The combined procedure had a positive effect on the regeneration of bone and cartilage on both sides of the joint [20–23].
Our early results with 16 patients have been reported elsewhere [24]. Ten of these patients have since reached skeletal maturity. Their functional clinical and radiographic assessments are described below.
Patients and methods
The operative technique has been described previously [24]. We used gradual distraction over a period of time rather than acute distraction on the operating table during surgery [23]. Of 16 patients who had undergone a combined surgical procedure of soft tissue release and joint distraction with a hinged mono-lateral external fixator in our department between 1999–2004 [24], 10 had reached skeletal maturity and comprise our current study group. They included eight boys and two girls whose mean age at surgery was 12.3 years (range 9.4–15.1). Their mean age at last follow-up was 18.1 years (range 15.2–22.8), and the mean follow-up was of 5.7 years (range 4.3–7.8). The study was approved by our institutional review board and registered with the ministry of health regulation with application no 920060515.
Clinical assessment
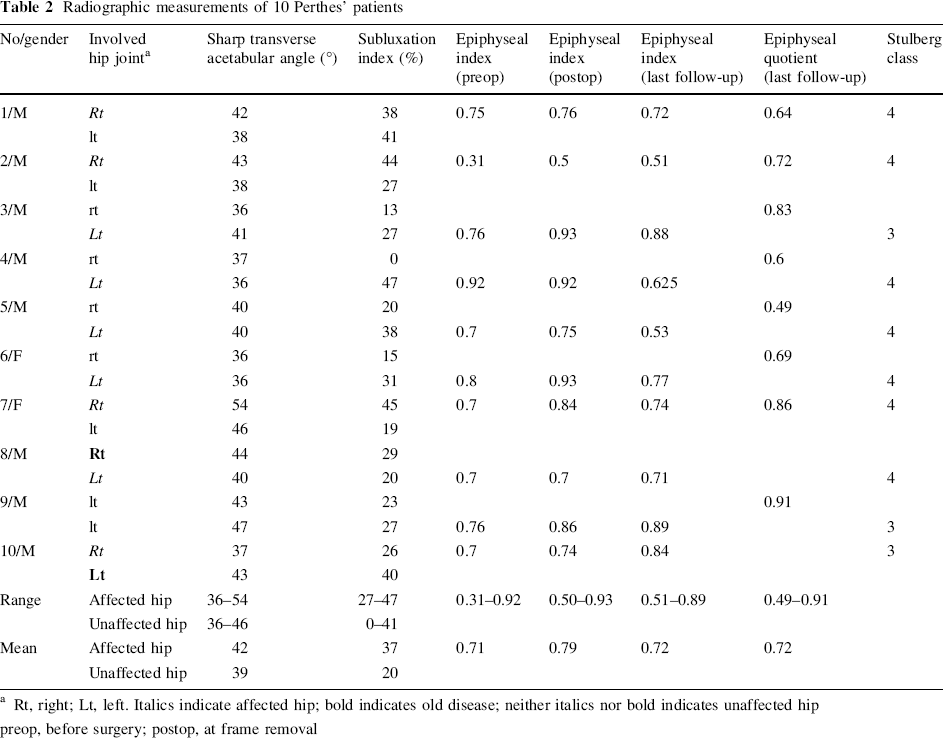
All the patients reported herein were interviewed and were asked to complete a questionnaire in person during their last outpatient visit. We calculated the Harris hip score for pain, function, daily activities, hip range of motion (ROM), and limb length discrepancy [25], and all patients completed the Oxford hip questionnaire for pain and function [26] (Table 1).
Clinical parameters of 10 Perthes’ patients
DOB, date of birth; FU, follow-up; ROM, range of motion; FFD, fixed flexion deformity; AB, abduction; IR, internal rotation; LLD, limb length discrepancy
Radiographic assessment
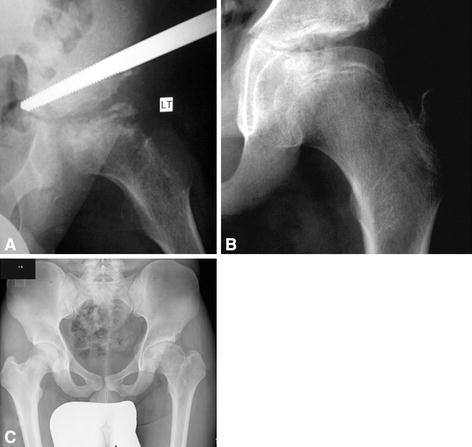
The radiographic measurements were done using the Orthocrat (OrthoCad Version 1.6) digital planning software. We measured the following parameters; the results are shown in Table 2.
Sharp transverse acetabular inclination for comparison of the ten affected hips to the eight unaffected hips. This is defined as the angle between a transverse pelvic line at the tip of the tear drop and the oblique line from this point to the superolateral corner of the acetabulum [27]. The uncoverage percentage (using Reimer's subluxation index) for comparison of the ten affected hips to the eight unaffected hips. This is defined as the percentage of the femoral head at the widest transverse diameter that protrudes laterally to Perkin's vertical line [27]. The epiphyseal index (Eyre–Brook modified by Tonnis) as assessed on arthrograms before surgery, at frame removal and on plain X-rays at last follow-up. This is defined as the ratio between the epiphyseal height at the midline point divided by the epiphyseal width at its widest points [27]. The value was multiplied by two for convenience of presentation; normal range for our age group is 0.8–0.9. The epiphyseal quotient (of Sjovall) on the last follow-up X-rays, defined as the epiphyseal index of the affected hip divided by the epiphyseal index of the unaffected hip. This is a measure of epiphyseal flatness compared to the unaffected side; normal range for our age group is 0.8–0.9.
Radiographic measurements of 10 Perthes’ patients
Rt, right; Lt, left. Italics indicate affected hip; bold indicates old disease; neither italics nor bold indicates unaffected hip preop, before surgery; postop, at frame removal
Statistical methods
The non-parametric Wilcoxon signed ranks test was used to compare the affected and the unaffected hips for differences in the acetabular inclination angle and subluxation index. Two cases were excluded from this analysis since both hip joints were involved. The non-parametric Wilcoxon signed ranks test was used to compare the epiphyseal index before surgery, at frame removal, and at last follow-up. Significance was set at P < 0.05.
Results
Clinical and functional outcome
The mean Harris hip score was 86.3/100 (range 48.5–96), with one patient scoring below 85 points. Six of the ten patients reported slight pain (40/44 points) after walking for more than an hour, but none was limited in walking distance. Most patients had some limitation of hip extension: the mean fixed flexion contracture was 6° (range 0–20), with 5° of extension on the unaffected side (range −10 to 10). The abduction was limited, with a mean of 28° (range 0–50) compared to 45° for the unaffected side (range 30–50). The mean internal rotation was 9° (range 0–15) compared to 40° for the unaffected side (range 35–45). Three of the ten patients had a limp due to limb shortening, and one of them had a positive Trendelenburg sign.
There was no limb length discrepancy in three patients; it was 1 cm in four patients and 2.5, 3.5, and 4 cm each in the remaining three patients. The latter three patients used shoe lifts (Table 1).
The mean score of the Oxford hip questionnaire was 17.4/60 (range 12–31). Six of the ten patients reported slight pain related to strenuous activity during the month preceding the last follow-up.
Radiographic evaluation
The mean Sharp transverse acetabular inclination for the ten affected hips was 42° (range 36–54) compared to a mean of 39° (range 36–46) for the eight unaffected hips (P < 0.045). The mean uncoverage percentage (using Reimer's subluxation index) for the ten affected hips was 37% (range 27–47) compared to a mean of 20% (range 0–41) for the eight unaffected hips (P < 0.017). The mean epiphyseal index (Eyre–Brook modified by Tonnis) before surgery was 0.71 (range 0.31–0.92), and it improved to a mean of 0.79 (range 0.50–0.93) at frame removal (P = 0.012). The results for the epiphyseal index at the last follow-up showed similar values to those before surgery (mean 0.72, range 0.51–0.89; P = 0.646). The epiphyseal quotient (Sjovall) for the eight unilateral cases was 0.72 (range 0.49–0.91). Three of the affected hips had a type III Stulberg classification and seven had a type IV (Figs. 1, 2; Table 2).

Discussion
Hip joint bony deformity and cartilage irregularity may lead to pain, arthritic changes, and stiffness. In Perthes’ disease the collapse of the femoral head during the avascular stage creates a deformed incongruent situation with increased stresses across the joint; this may eventually result in early degenerative changes. In order to prevent degeneration of the joint, different treatment strategies have been offered. Reports on the value of hip distraction appeared in the early nineties and again recently when it was applied to stiff hips with Perthes’ disease and to other conditions with joint surface irregularity [20, 23].
The effect of arthrodiastasis is to reduce the pressure across the joint and, combined with ROM exercises, to provide nourishment to the joint cartilage and improve regeneration. Joseph et al. [1] recommended that treatment should be started before epiphyseal collapse had occurred, since the potential to remodel in the older age group children is limited. Maxwell et al. [30] applied the articulated distractor to hips with minimal collapse in order to maintain epiphyseal height. They reported early results with preservation of epiphyseal height and arrest of epiphyseal collapse.
Thacker et al. used an articulated distractor to treat patients with osteonecrosis and joint space narrowing. All their patients had constant pain and limited ROM, both of which improved after a mean duration of 4.4 months with the fixator. Although joint space widened from a mean of 2.6 mm to a mean of 4.8 mm, there was significant deterioration compared to the immediate postoperative period at latest follow-up [23].
We present our results with the distraction technique at skeletal maturity. Improvement in pain could be attributed to the late stage of the disease with accompanying reduction of the inflammatory changes and may not reflect a better outcome compared to other treatments. Our early results [24] had shown improvement of head sphericity at frame removal, but the values we now measured at skeletal maturity were similar to the preoperative ones. This deterioration may reflect the possibility that the regenerated femoral head is less resistant to normal stresses across the joint. Although the overall clinical satisfaction from this treatment was high, the radiographic results for head uncoverage and epiphyseal index did not improve significantly.
We did not perform any additional surgery on the acetabulum after the distraction procedure. Theoretically, such surgery can still be performed and we will consider additional surgery should there be any indication for it.
Our results are comparable to those of the established method of valgus extension osteotomy as a salvage procedure for hinge abduction. Two recent papers reported significant clinical improvement following osteotomy, i.e., an average Iowa hip score of 86 for 51 operated hips [31] and an average score of 92 for 21 operated hips [32]. The radiographic results were, however, again less favorable, i.e., Stulberg class IV and V in 53% [31] and III and IV in 85.7% [32], results that are similar to the outcome for our patients.
The above-cited clinical and radiographic results may be compared and used as a reference for conservative or surgical treatment outcome in children with late-onset Perthes’ disease as they reach the important stage of skeletal maturity.
According to our experience we apply this treatment protocol to:
late onset disease, that is a skeletal age of 9 years or older; radiographic evidence of collapse of the lateral pillar with hinge abduction, narrow joint space and established deformity; and severe limitation of hip range of motion and pelvic obliquity.
We believe that combined soft tissue release and articulated hip distraction can be regarded as a salvage procedure without compromising the possibility for future surgery.